I've been asked a few times about this slide so here's a thread about where it comes from, what it means, and why we should take it seriously.
My argument is that the patients we look after and their families that we talk to approach sudden bad events with expectations informed by what they have seen.
Our outcome expectations are also informed by what we have seen. The difference is they are likely to have seen it on TV; we are likely to have seen it in emergency departments & intensive care units.
There is a gap. Recognising this is an essential skill in managing expectations & breaking bad news. Families aren't stupid. They aren't going to say 'but the man off the telly survived'. But what they have seen will influence expectation & response.
So not only is it good that as clinicians we are aware of this gap, but we also get to watch lots of TV shows & claim it was 'research'. They highlight some interesting cultural differences too. So, let's begin...
Here's one from Resuscitation in 2009.
pubmed.ncbi.nlm.nih.gov/19699021-resus…
It's a British study. They watched 88 episodes of 2 UK & 2 US medical dramas & noted all those who received CPR. The outcomes measures were immediate survival & survival to discharge.
pubmed.ncbi.nlm.nih.gov/19699021-resus…
It's a British study. They watched 88 episodes of 2 UK & 2 US medical dramas & noted all those who received CPR. The outcomes measures were immediate survival & survival to discharge.
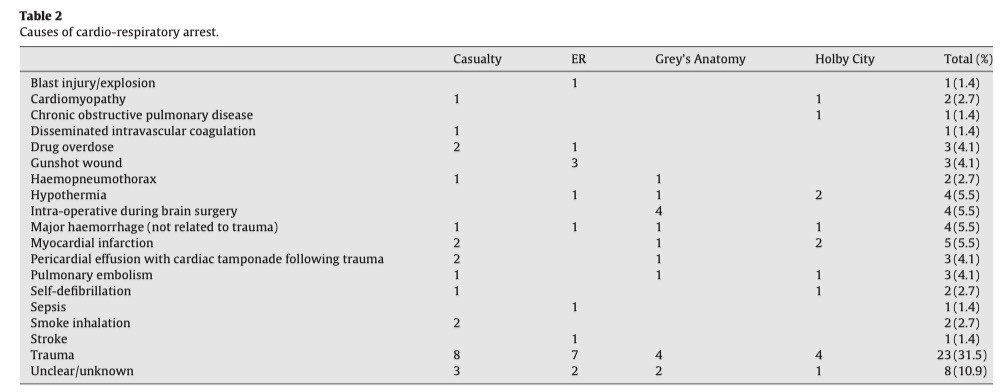
In 88 episodes there were 76 cardio-respiratory arrests with 70 resuscitation attempts. This was 0.86 arrests per episode.
The most common preceding event was trauma (31%). Consistent with trauma, but absolutely inconsistent with IHCAs, the average age of cardiac arrest was 36.
The most common preceding event was trauma (31%). Consistent with trauma, but absolutely inconsistent with IHCAs, the average age of cardiac arrest was 36.

Immediate survival was 46%. The reality (for traumatic cardiac arrest) is 5-7% (resuscitationjournal.com/article/S0300-…) . Long term-survival was unclear; most showed full recovery or death. There was little suggestion of hypoxic ischaemic brain injury.
The authors conclude that viewers of these programmes are likely to conclude the survival of a 75 year-old OHCA is the same as a 25 year-old given the absence of portrayal of age-related decline.
Let's move on to coma.


These authors deserve a special mention for going above and beyond by watching 9 daytime US soap operas over an 11 year period that contained references to coma.
The titles alone stand as a tribute to the researcher's self-sacrifice:
"Guiding Light, General Hospital, One Life to Live, Days of Our Lives, All My Children, Passions, As the World Turns, The Young and the Restless, and The Bold and the Beautiful."
"Guiding Light, General Hospital, One Life to Live, Days of Our Lives, All My Children, Passions, As the World Turns, The Young and the Restless, and The Bold and the Beautiful."
They found 64 characters with periods of unconsciousness lasting a minimum of 24 hours. The coma was followed through to its conclusion (recovery, death or last appearance). The cause of coma was ascertained from storyline review from fan or official websites.
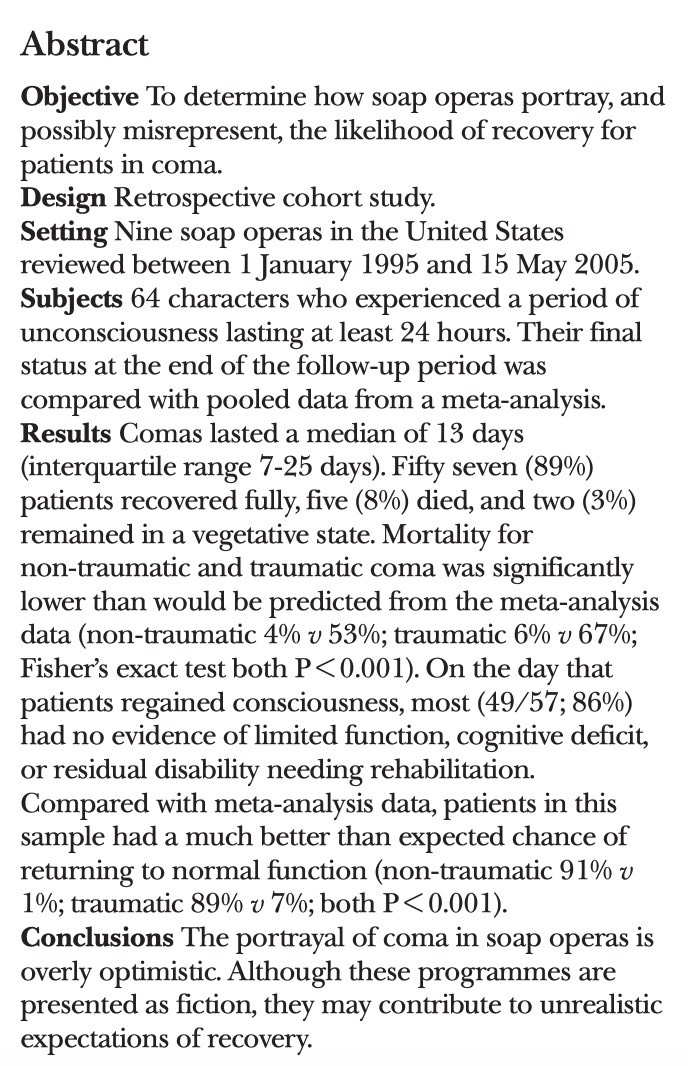
Of 73 comas, 6 were excluded. One woke for meals (!), two were faking it, and 3 were drug-induced.
Median coma duration was 13 days (IQR 7-25).
89% recovered fully.
8% died
3% remained in vegetative state to follow-up
Median coma duration was 13 days (IQR 7-25).
89% recovered fully.
8% died
3% remained in vegetative state to follow-up
Here's one of the best exclusion criteria you are ever likely to read in a major journal.

Followed by a qualifier that is also unlikely to appear in many other papers.
Of those who regained consciousness, 86% had no residual disability on the day of (suddenly) waking. Those with (disorientation, amnesia) subsequently rapidly made a full recovery.
So what does this mean? Like CPR, the vast majority of comatose patients were portrayed as making a full, often instant, recovery. 64% of comas portrayed were traumatic in origin. Family expectations are very unlikely to align with actual outcomes.

And now on to my favourite one, if only for the methods, being a retrospective study of future events
pubmed.ncbi.nlm.nih.gov/25457378-where…
pubmed.ncbi.nlm.nih.gov/25457378-where…
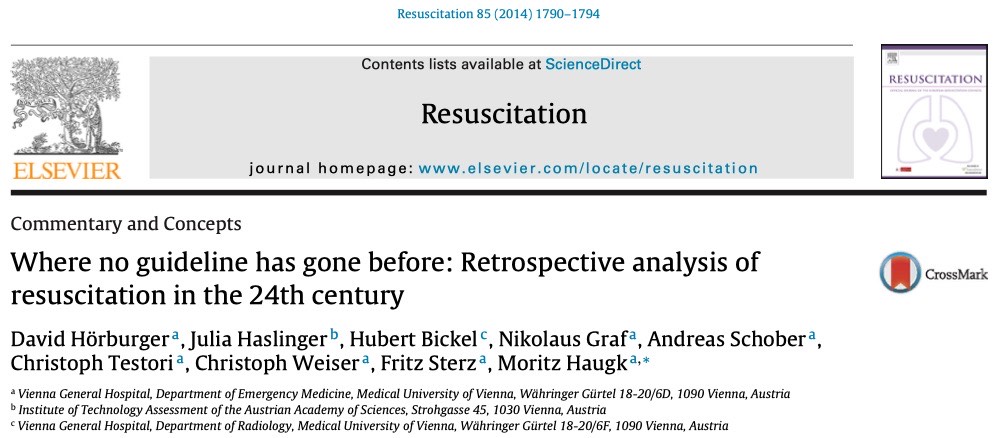
The entire modern Star Trek canon (526 episodes) was examined for cardiac arrests, resulting in the identification of 163 episodes which were watched to enable analysis of management.
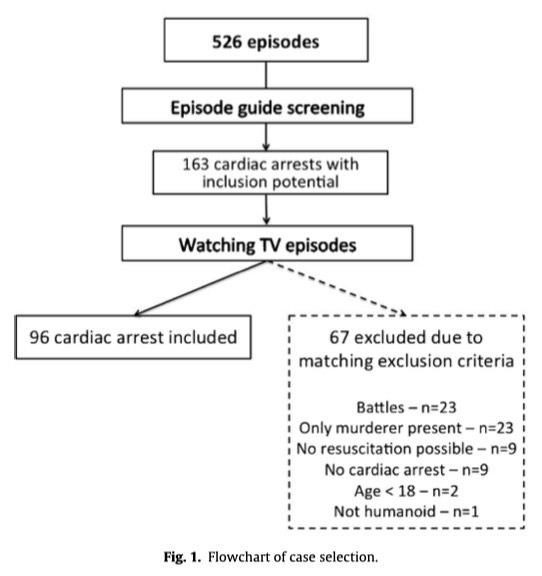
As with the coma paper, the exclusion criteria are unique.
'Only murderer present' & 'not humanoid' don't appear in many CPR outcome analysis papers.
'Only murderer present' & 'not humanoid' don't appear in many CPR outcome analysis papers.
So, some bad news. The future seems to be quite violent. And energy weapons are a common cause of cardiac arrest.
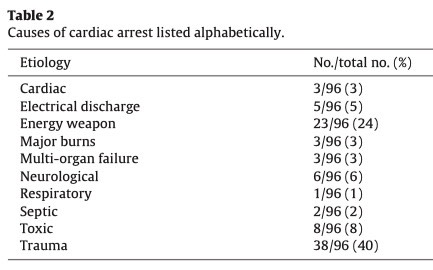
And more bad news, the survival of cardiac arrest in the future is abysmal, despite almost every arrest being witnessed. Defibrillation & drug administration rates were appalling. And it seems that mild hypothermia never made it into future guidelines.
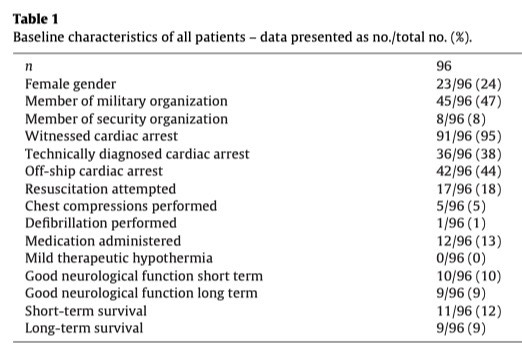
The absence of ECMO-CPR is striking, suggesting that CHEER-2 (or whatever its going to be called) was an abysmal failure (HT @precordialthump & The Alfred crew).
@precordialthump The discussion of this paper is worth reading only because the authors are clearly Very Serious about Star Trek and I admire anyone of ascends to this level of Geekery especially given their admirable review of contemporary Starfleet literature.
Just in case anyone's still reading, I'll add some more later.
Web browser crash broke thread. Rejoining: