The words HERD IMMUNITY are bastardised - BigBrother Newspeak 1984
You do NOT get HERD IMMUNITY exposing the population. The OPPOSITE. You vaccinate everyone to ensure they are NOT exposed.
A Perversion - kill the MANY to help THE FEW.
Thanos😱😈⬇️
You do NOT get HERD IMMUNITY exposing the population. The OPPOSITE. You vaccinate everyone to ensure they are NOT exposed.
A Perversion - kill the MANY to help THE FEW.
Thanos😱😈⬇️
Herd 2/7
Let's imagine we change #Covid19, and replace it with SmallPox.
Now Patrick Vallance says, we need to create herd immunity in the UK by slowly letting SmallPox spread through the population.
Feeling good about that?
Trolls now say I chose a sensationalist disease:
Let's imagine we change #Covid19, and replace it with SmallPox.
Now Patrick Vallance says, we need to create herd immunity in the UK by slowly letting SmallPox spread through the population.
Feeling good about that?
Trolls now say I chose a sensationalist disease:
Herd 3/7
That's because they're muppets.
Smallpox is relevant because
a) we let it spread - for about 900 years,
b) it was the first disease we created a vaccine for,
c) it is the ONLY disease irradicated through ONLY vaccines
who.int/csr/disease/sm…
That's because they're muppets.
Smallpox is relevant because
a) we let it spread - for about 900 years,
b) it was the first disease we created a vaccine for,
c) it is the ONLY disease irradicated through ONLY vaccines
who.int/csr/disease/sm…
Herd 4/7
Human beings never gained herd immunity from Smallpox by letting it spread or
polio
flu
colds
typhoid
hepatitis
HIV
Measles Mumps Rubella
Need I go on?
The reason we didn't was there is no herd immunity based on exposure - the whole concept is based on immunisation
Human beings never gained herd immunity from Smallpox by letting it spread or
polio
flu
colds
typhoid
hepatitis
HIV
Measles Mumps Rubella
Need I go on?
The reason we didn't was there is no herd immunity based on exposure - the whole concept is based on immunisation
Herd 5/7
And you know that's true because of, ironically, the deeply toxic antivax memes that have created the mess in the US⬇️
Ever heard anyone say Measles - It's ok, we have herd immunity, stop vaccinating?
Of course not. You've heard the opposite.
en.wikipedia.org/wiki/Measles_r…
And you know that's true because of, ironically, the deeply toxic antivax memes that have created the mess in the US⬇️
Ever heard anyone say Measles - It's ok, we have herd immunity, stop vaccinating?
Of course not. You've heard the opposite.
en.wikipedia.org/wiki/Measles_r…
Herd 6/7
I do not know how Sir Patrick Vallance ends up saying things that are
a) Not valid science
b) In contradiction to the WHO guidelines
c) directly opposing advice from countries better prepared, experienced and with more success than us
But he has
I do not know how Sir Patrick Vallance ends up saying things that are
a) Not valid science
b) In contradiction to the WHO guidelines
c) directly opposing advice from countries better prepared, experienced and with more success than us
But he has
Herd 7/7
Look at Vietnam, Singapore, even China, to know how the answer is STOP mass spread or
Italy "don't do what we did"
What do I know? Im no epidemiologist, but i can claim research on Zidovudin (HIV antiviral), and I've added links to all sources in thread.
UKGov has not
Look at Vietnam, Singapore, even China, to know how the answer is STOP mass spread or
Italy "don't do what we did"
What do I know? Im no epidemiologist, but i can claim research on Zidovudin (HIV antiviral), and I've added links to all sources in thread.
UKGov has not
@threadreaderapp unroll
Herd 8/tbd
I'm alarmingly encountering twitter bots/trolls reinforcing the Government's interpretation of #herdimmunity, advocating "benefits".
I hope if there are trials, the accounts of Governmental Advisers are checked.
so let's get into the invalidity of those arguments
I'm alarmingly encountering twitter bots/trolls reinforcing the Government's interpretation of #herdimmunity, advocating "benefits".
I hope if there are trials, the accounts of Governmental Advisers are checked.
so let's get into the invalidity of those arguments
Herd 9/
I'll cover
1. Is Herd Immunity (HI) achieved by immunisation, the same as HI by exposure?
2. Can you achieve HI by exposure?
3. Is HI by exposure preferable
a) to by immunisation
b) if you don't have immunisation to any other regime?
I think that'll do it.
I'll cover
1. Is Herd Immunity (HI) achieved by immunisation, the same as HI by exposure?
2. Can you achieve HI by exposure?
3. Is HI by exposure preferable
a) to by immunisation
b) if you don't have immunisation to any other regime?
I think that'll do it.
H10/
IMMUNISATION VS EXPOSURE
IMMUNISATION - most of the diseases I listed above have vaccines and they work because in some cases, of years, tracking down the last case.
But the reason for including the measles example is it's not perfect reduce coverage below X%, problems
IMMUNISATION VS EXPOSURE
IMMUNISATION - most of the diseases I listed above have vaccines and they work because in some cases, of years, tracking down the last case.
But the reason for including the measles example is it's not perfect reduce coverage below X%, problems
H11/
But not all diseases can be treated like this - and there are a few reasons for that.
Sometimes the vaccine is really really hard to find
In other cases the disease changes so quickly it's hard to keep up
Still others have so many versions, you can't get them all
But not all diseases can be treated like this - and there are a few reasons for that.
Sometimes the vaccine is really really hard to find
In other cases the disease changes so quickly it's hard to keep up
Still others have so many versions, you can't get them all
H12/
So, for example, the flu is like number 2 and the reason the winter flu vaccine is so ineffective, is the flu changes so fast
Number 3 is HIV, not only was that hard to find, we had to invent a way to attack the virus from multiple directions to contain it
So, for example, the flu is like number 2 and the reason the winter flu vaccine is so ineffective, is the flu changes so fast
Number 3 is HIV, not only was that hard to find, we had to invent a way to attack the virus from multiple directions to contain it
H13
And number 1 (with a bit of 2 thrown in) is the common cold. Despite working on this since the 1950s, we haven't solved it (I think we never will) because it is mainly two viruses, but each of those have many versions
The two? Rhinovirus and.... Coronovirus
And number 1 (with a bit of 2 thrown in) is the common cold. Despite working on this since the 1950s, we haven't solved it (I think we never will) because it is mainly two viruses, but each of those have many versions
The two? Rhinovirus and.... Coronovirus
H14/
Yes, we do know this virus - in fact, you heard people calling it "novel" because it was a new version.
And these examples show that no-one can guarantee at the start a vaccine for any specific disease.
They can hope, and estimate, but until the work starts...
Yes, we do know this virus - in fact, you heard people calling it "novel" because it was a new version.
And these examples show that no-one can guarantee at the start a vaccine for any specific disease.
They can hope, and estimate, but until the work starts...
H15/
That was immunisation (btw not same as vaccination see below). If you have a vaccine and if it's stable and if you can deploy it, and if people keep taking it, you can achieve herd immunity - the point at which even if a few people aren't immune, the herd stays safe.
That was immunisation (btw not same as vaccination see below). If you have a vaccine and if it's stable and if you can deploy it, and if people keep taking it, you can achieve herd immunity - the point at which even if a few people aren't immune, the herd stays safe.

H16/
HI By Exposure
In the next section, you'll find out why it's hard to assess if you can achieve the same effect via exposure.
But this section asks if they are the same.
Clearly they aren't
Immunisation grows a vaccinated population over time.
Then deploys vaccine to kids
HI By Exposure
In the next section, you'll find out why it's hard to assess if you can achieve the same effect via exposure.
But this section asks if they are the same.
Clearly they aren't
Immunisation grows a vaccinated population over time.
Then deploys vaccine to kids
H17
Exposure based HI would need you to actively infect almost everyone in order to create the same high level of cover as vaccination.
But then if not vaccine was found, you'd need to expose kids to the virus quickly and early - think chickenpox parties.
But...it's worse
Exposure based HI would need you to actively infect almost everyone in order to create the same high level of cover as vaccination.
But then if not vaccine was found, you'd need to expose kids to the virus quickly and early - think chickenpox parties.
But...it's worse
H18/
The reason we don't do flu parties is the same as the reason we have no herd immunity for the flu or stable vaccine.
The strain mutates so can't create immunity. So, you could only get Herd Immunity to work through exposure IF the virus was stable
is Coronovirus stable?
The reason we don't do flu parties is the same as the reason we have no herd immunity for the flu or stable vaccine.
The strain mutates so can't create immunity. So, you could only get Herd Immunity to work through exposure IF the virus was stable
is Coronovirus stable?
H19/
I'll be cautious, I'm not a lab scientist, I don't have the data the Government has.
But I know the category and I'm unaware of any mass population viruses in that category that have stable vaccines.
So we're going to need to be very lucky.
I'll be cautious, I'm not a lab scientist, I don't have the data the Government has.
But I know the category and I'm unaware of any mass population viruses in that category that have stable vaccines.
So we're going to need to be very lucky.
H20/
Question 1 - Is HI from immunisation or Exposure the same?
No, not mechanism and deployment,
Not even the outcome, depending on vaccination availability, the same.
AND it's likely if you can't make a vaccine, exposure won't work anyway due to mutation.
Question 1 - Is HI from immunisation or Exposure the same?
No, not mechanism and deployment,
Not even the outcome, depending on vaccination availability, the same.
AND it's likely if you can't make a vaccine, exposure won't work anyway due to mutation.
H21/
Question 2 Can we achieve HI through Exposure for #corvid19?
The obvious thing is look up successful exposure-based #herdimmunity examples on google.
Did you find any?
I'm unaware of any. No one has ever tried. Nor as we'll into in 3, can I think of a reason they would
Question 2 Can we achieve HI through Exposure for #corvid19?
The obvious thing is look up successful exposure-based #herdimmunity examples on google.
Did you find any?
I'm unaware of any. No one has ever tried. Nor as we'll into in 3, can I think of a reason they would
H22/33 So it's hard to answer if you could, but you know already the virus must be a) stable, and b) deployable quickly, because if you're slow, even stable viruses mutate.
If the UK Gov has that information, they haven't shared it. I think the W.H.O. would be angry about that.
If the UK Gov has that information, they haven't shared it. I think the W.H.O. would be angry about that.
H23/33
But it's a little worse. You see the % at which HI works isn't an exact science, I've seen UKGov bots online saying it's 60%.
For the reasons given above, I cannot prove to you that it isn't. But you know already since no-one has done this, they can't know either.
But it's a little worse. You see the % at which HI works isn't an exact science, I've seen UKGov bots online saying it's 60%.
For the reasons given above, I cannot prove to you that it isn't. But you know already since no-one has done this, they can't know either.
H24/33
let's imagine it's more like the standard 95%
And just half of our old people are self - isolating, ie NOT EXPOSED
Are we going to pull them out of their homes to have coronavirus "parties" to ensure we get to the right exposure rate?
How very Josef Mengele
let's imagine it's more like the standard 95%
And just half of our old people are self - isolating, ie NOT EXPOSED
Are we going to pull them out of their homes to have coronavirus "parties" to ensure we get to the right exposure rate?
How very Josef Mengele
H25/33
Question 2 Can we achieve HI through Exposure for #corvid19?
You would have to be very brave, very informed, or out of options to try. Because I can't see any way that you can know, today, that it'll work. And, as you'll see, I can see many disadvantages.
Question 2 Can we achieve HI through Exposure for #corvid19?
You would have to be very brave, very informed, or out of options to try. Because I can't see any way that you can know, today, that it'll work. And, as you'll see, I can see many disadvantages.
H26/33
Time for the final question
3. Is HI by exposure preferable
a) by immunisation
b) if you don't have immunisation to any other regime?
I hope you can see that part 3a) is now easy to answer. Why would you? If you have a valid vaccine you'd get that out as fast as possible
Time for the final question
3. Is HI by exposure preferable
a) by immunisation
b) if you don't have immunisation to any other regime?
I hope you can see that part 3a) is now easy to answer. Why would you? If you have a valid vaccine you'd get that out as fast as possible
H27/33
AND
rather than exposing people
you'd SLOW exposure to create more vaccine and to manage NHS demand.
So how about 3b) what if you have no vaccine, and people are dying, would you try for #herdimmunity by a sort of Spock "needs of the many outways the few" argument?
AND
rather than exposing people
you'd SLOW exposure to create more vaccine and to manage NHS demand.
So how about 3b) what if you have no vaccine, and people are dying, would you try for #herdimmunity by a sort of Spock "needs of the many outways the few" argument?
H28/33
I feel dear twitter reader, you can answer that yourself, but for the record, it's hard to answer yes.
Here are the CONS
You don't know the stability
You don't know exposure success
You do know huge impact on NHS
And form my other thread you know death rate
I feel dear twitter reader, you can answer that yourself, but for the record, it's hard to answer yes.
Here are the CONS
You don't know the stability
You don't know exposure success
You do know huge impact on NHS
And form my other thread you know death rate
H29/33
That thread is linked above in the first tweet, but I post the relevant tweet here to make this easy.
Maybe I'm just not cut out for the big decisions, but I'd have to feel really good that a 5-15% death rate for anyone over 60 was worth it.
That thread is linked above in the first tweet, but I post the relevant tweet here to make this easy.
Maybe I'm just not cut out for the big decisions, but I'd have to feel really good that a 5-15% death rate for anyone over 60 was worth it.
H30/33
Ok so here are the PROs
I don't have any. I really want to find some, because if I don't, I look like I'm nagging. So just for the look of it...erm
Cover up containment mistakes?
That's it. If this thing is stable enough for Exposure HI, then we'll make a vaccine
Ok so here are the PROs
I don't have any. I really want to find some, because if I don't, I look like I'm nagging. So just for the look of it...erm
Cover up containment mistakes?
That's it. If this thing is stable enough for Exposure HI, then we'll make a vaccine
H31/33
If it's not stable enough, then it won't achieve HI, and it'll be with us forever.
But rushing towards that is a bad plan - we want to walk as slowly as possible, just to manage regimen learnings and NHS pressure.
Anything else is?
God knows - nuts?
If it's not stable enough, then it won't achieve HI, and it'll be with us forever.
But rushing towards that is a bad plan - we want to walk as slowly as possible, just to manage regimen learnings and NHS pressure.
Anything else is?
God knows - nuts?
H32/33
In summary (for #corvid19 not any other virus)
Is #herdimmunity by immunisation the same as by exposure NO NO and NO
Can you achieve #herdimmunity via exposure
VERY UNLIKELY
Do you wish to achieve #herdimmunity via exposure vs. any other treatment
ALMOST CERTAINLY NOT
In summary (for #corvid19 not any other virus)
Is #herdimmunity by immunisation the same as by exposure NO NO and NO
Can you achieve #herdimmunity via exposure
VERY UNLIKELY
Do you wish to achieve #herdimmunity via exposure vs. any other treatment
ALMOST CERTAINLY NOT
H33/33
So I find myself in exactly the same place as I was at the start of the thread, asking what the hell the UKGov is doing.
It was bad enough not to have any rationale for #Brexit
But no rationale for stuff that might kill my parents?
Now I'm seething
#WarCrimes
So I find myself in exactly the same place as I was at the start of the thread, asking what the hell the UKGov is doing.
It was bad enough not to have any rationale for #Brexit
But no rationale for stuff that might kill my parents?
Now I'm seething
#WarCrimes
H35/70
Update to review l the UKGov "strategy"
For context this is a strategy that has almost no published explanation or basis
It's one that has ignored WHO advice. AND deliberately failed containment exposing 100s of thousands quicker at random.
Better be good
Update to review l the UKGov "strategy"
For context this is a strategy that has almost no published explanation or basis
It's one that has ignored WHO advice. AND deliberately failed containment exposing 100s of thousands quicker at random.
Better be good
H36/70
So as probably THE most risky epidemiological "experiment" in history, I'll take each line of the guidance, with citations one by one so I can take you through the thinking.
Oh. Wait.
This experiment on millions has no published guidance or explanation.
Erm.
So as probably THE most risky epidemiological "experiment" in history, I'll take each line of the guidance, with citations one by one so I can take you through the thinking.
Oh. Wait.
This experiment on millions has no published guidance or explanation.
Erm.
H37/70
I'll take a risk. I'll take you through my "understanding" of the approach. This isn't easy since I can't advocate for this approach, but what else do we have?
So: Explanation by stage, followed by criticism for both strategies
Lots to say. Sorry. But it's important.
I'll take a risk. I'll take you through my "understanding" of the approach. This isn't easy since I can't advocate for this approach, but what else do we have?
So: Explanation by stage, followed by criticism for both strategies
Lots to say. Sorry. But it's important.
H38/70
1.1 DEFINITIONS
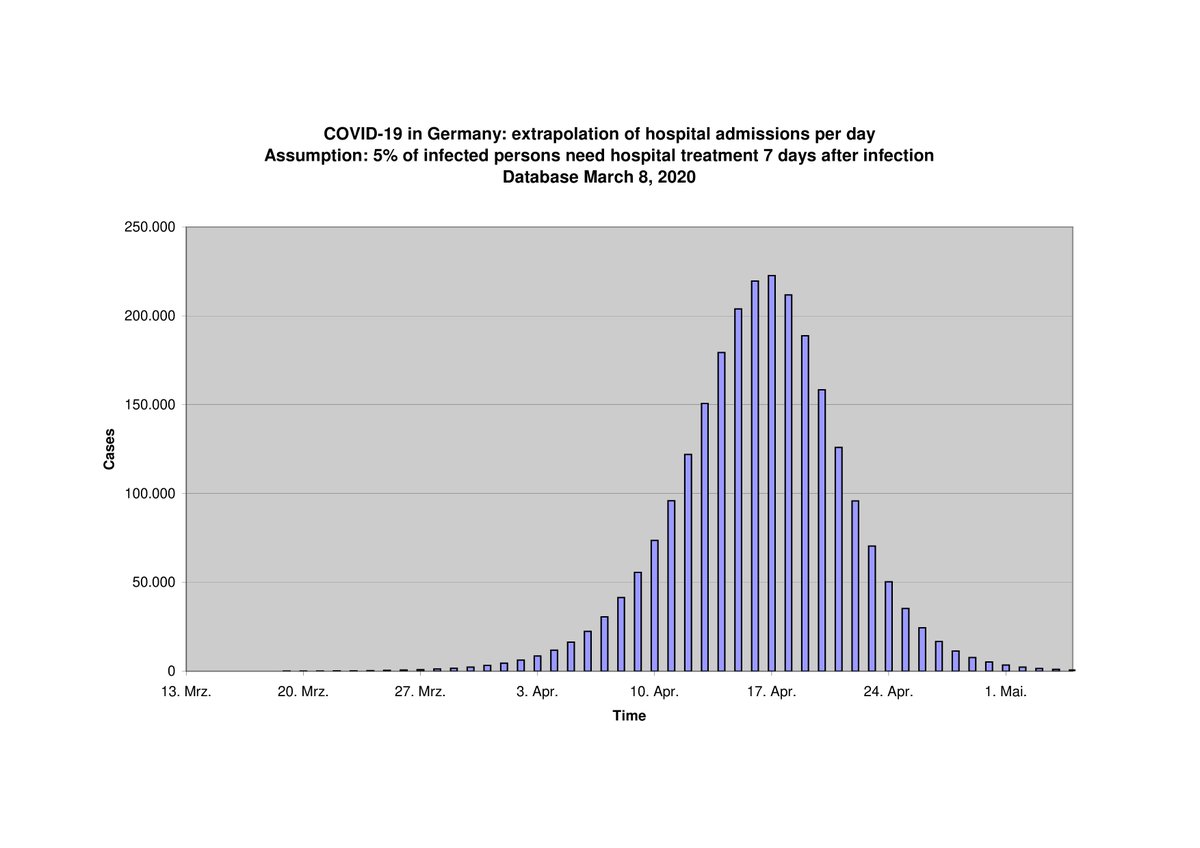
WHO strategy used successful countries' delay strategy. Delay the viral onset to give time to treat and not to overwhelm medical services.
UK Gov keeps objectives but speeds up the exposure in less risky groups to "save" higher risk. It's based on theory
1.1 DEFINITIONS
WHO strategy used successful countries' delay strategy. Delay the viral onset to give time to treat and not to overwhelm medical services.
UK Gov keeps objectives but speeds up the exposure in less risky groups to "save" higher risk. It's based on theory
H39/70
High risk self isolate during the "speed"
There is/was a 2nd mechanism - like bellows on a fire. A plan to heat up or slow down the virus by allowing and then banning, sequentially public gatherings to get less at risk infected. And to use a similar mechanism in schools.
High risk self isolate during the "speed"
There is/was a 2nd mechanism - like bellows on a fire. A plan to heat up or slow down the virus by allowing and then banning, sequentially public gatherings to get less at risk infected. And to use a similar mechanism in schools.
H40/70
There is/was because that's unclear now, with the Government reversing it. At least for mass gatherings. Unclear for schools.
Typically changing your deployment in the second day is not a good indicator.
And providing no guidance for a high logistical effort?
There is/was because that's unclear now, with the Government reversing it. At least for mass gatherings. Unclear for schools.
Typically changing your deployment in the second day is not a good indicator.
And providing no guidance for a high logistical effort?
H41/70
1.2 CRITICISM
You see some problems immediately.
Delay works if you act quickly as they did in Asia and as Italy very firmly told us to do.
If you act slowly, or God Help us, actively decide not to do containment without telling anyone it will be less effective.
1.2 CRITICISM
You see some problems immediately.
Delay works if you act quickly as they did in Asia and as Italy very firmly told us to do.
If you act slowly, or God Help us, actively decide not to do containment without telling anyone it will be less effective.
H42/70
Not ineffective, particularly with isolation, but you must be fast. Which is why many were screaming last week at the ineptitude of UKGov⏬
This now seems to be intentional and incredibly risky. And IMO even for the Gov strategy unnecessary.
Not ineffective, particularly with isolation, but you must be fast. Which is why many were screaming last week at the ineptitude of UKGov⏬
This now seems to be intentional and incredibly risky. And IMO even for the Gov strategy unnecessary.
H43/70
The Gov strategy. We'll get into details, but just on what's in the summary, you see it's complicated logistics.
A bunch of people have to isolate. The rest have to expose willingly, including (or not) occasional mass gathering. And then we're going to use your kids.
The Gov strategy. We'll get into details, but just on what's in the summary, you see it's complicated logistics.
A bunch of people have to isolate. The rest have to expose willingly, including (or not) occasional mass gathering. And then we're going to use your kids.
H44/70
This has challenging logistics all over it.
But I think the bigger problem is psychology.
At the best of times it's hard to persuade people to infect themselves intentionally.
But to ask them to expose their kids?
There's a myth the young don't get covid...
This has challenging logistics all over it.
But I think the bigger problem is psychology.
At the best of times it's hard to persuade people to infect themselves intentionally.
But to ask them to expose their kids?
There's a myth the young don't get covid...
H45/70
They do. Just at lower rates, and they die, at lower rates. But still 20x the rate of flu (data below).
Call me a snowflake but a plan that requires parents to willingly expose their kids, even at very low death rates, had colossal warning signs.
They do. Just at lower rates, and they die, at lower rates. But still 20x the rate of flu (data below).
Call me a snowflake but a plan that requires parents to willingly expose their kids, even at very low death rates, had colossal warning signs.
H46/70
2.1 Assumptions.
WHO/Delay has no relevant assumptions I can think of, beyond attempting the delay, which we deliberately didn't do.
UKGov assumes the virus will eventually expose the whole population on the argument you can only slow not stop it. So manage it instead.
2.1 Assumptions.
WHO/Delay has no relevant assumptions I can think of, beyond attempting the delay, which we deliberately didn't do.
UKGov assumes the virus will eventually expose the whole population on the argument you can only slow not stop it. So manage it instead.
H47/70
2.2 CRITICISM
The obvious problem with WHO/Delay is if you fail to delay, by accident (italy) or design (UK) you risk overwhelming exposure you cant control.
But Italy is worst case scenario and UK was NOT in the same situation. Plus Vietnam, SG and China are successes.
2.2 CRITICISM
The obvious problem with WHO/Delay is if you fail to delay, by accident (italy) or design (UK) you risk overwhelming exposure you cant control.
But Italy is worst case scenario and UK was NOT in the same situation. Plus Vietnam, SG and China are successes.
H48/70
So you can't assume delay won't work. If anything you can see very clearly how Italy was exposed and Asia was not and make sure you follow Asia.
And use the 1000 of words of advice, guidelines, systems and medical regimen provided by the World Health Organisation.
So you can't assume delay won't work. If anything you can see very clearly how Italy was exposed and Asia was not and make sure you follow Asia.
And use the 1000 of words of advice, guidelines, systems and medical regimen provided by the World Health Organisation.
H49/70
Or you can go it alone ignoring all countries who've been fighting SARs for a decade (a close relative of covid) with a strategy that is theoretical but has never been tried.
And which needs precision logistics and psychology.
Like lighting a candle with a flamethrower.
Or you can go it alone ignoring all countries who've been fighting SARs for a decade (a close relative of covid) with a strategy that is theoretical but has never been tried.
And which needs precision logistics and psychology.
Like lighting a candle with a flamethrower.
H50/70
And you've made a huge assumption - covid will infect everyone (Asia disproves this for now)
And you've taken a vast risk. Instead of containing you've thrown open the doors. Including to airlines coming from Italy?
You should expect almost random infection which we have
And you've made a huge assumption - covid will infect everyone (Asia disproves this for now)
And you've taken a vast risk. Instead of containing you've thrown open the doors. Including to airlines coming from Italy?
You should expect almost random infection which we have
H51/70
And you do all this containment sabotage at the same time that Italy is categorically telling you whatever you do
1) follow WHO advice
2) do not under any circumstances delay containment.
Maybe as experienced China you could try. But as UK?
And you do all this containment sabotage at the same time that Italy is categorically telling you whatever you do
1) follow WHO advice
2) do not under any circumstances delay containment.
Maybe as experienced China you could try. But as UK?
H52/70
3.1 Management
Delay does what it can. It slows exposure and manages the population through. At this point no one knows what that will entail because we don't know how the virus will behave.
If it's SARS, you may be able to wipe it out. If it's a cold, it's coming back.
3.1 Management
Delay does what it can. It slows exposure and manages the population through. At this point no one knows what that will entail because we don't know how the virus will behave.
If it's SARS, you may be able to wipe it out. If it's a cold, it's coming back.
H53/70
Gov theoretically manages supply and demand - you encourage low risk people to get infected, or you use your large crowds or school bellows to infect. Then as hospitals fill you dial back.
Your aim is to do this in cycles like a wave. Making sure hospitals aren't filled
Gov theoretically manages supply and demand - you encourage low risk people to get infected, or you use your large crowds or school bellows to infect. Then as hospitals fill you dial back.
Your aim is to do this in cycles like a wave. Making sure hospitals aren't filled
H54/70
You control your estimates of infection rate with models and you c update data with the relative mild vs severe infected rate - it's the severe which can overwhelm you.
Meanwhile anyone high risk is self isolating until all of the low risk have infected and recovered.
You control your estimates of infection rate with models and you c update data with the relative mild vs severe infected rate - it's the severe which can overwhelm you.
Meanwhile anyone high risk is self isolating until all of the low risk have infected and recovered.
H55/70
3.2 CRITISCISM
There are some big problems for both strategies here. With Delay it's possible you need very large amounts of people under lock down for long periods.
That will be unsustainable, though viral infection is a good shield against none compliance!
3.2 CRITISCISM
There are some big problems for both strategies here. With Delay it's possible you need very large amounts of people under lock down for long periods.
That will be unsustainable, though viral infection is a good shield against none compliance!
H56/70
Delay is by definition a holding strategy. BUT if it's not SARS and immunity is only as long as the next major mutation, you are going to need to face what you do - infection of unexposed and re-exposed.
No one knows yet how that will play out, including our Government.
Delay is by definition a holding strategy. BUT if it's not SARS and immunity is only as long as the next major mutation, you are going to need to face what you do - infection of unexposed and re-exposed.
No one knows yet how that will play out, including our Government.
H57/70
GoV
This balancing you have to do keeping infection rates in line with hospital capacity is incredibly complex.
Even beyond the discussed psychological and logistics issues human beings are unpredictable. You have to get this right at the town level. With good compliance
GoV
This balancing you have to do keeping infection rates in line with hospital capacity is incredibly complex.
Even beyond the discussed psychological and logistics issues human beings are unpredictable. You have to get this right at the town level. With good compliance
H58/70
Plus the virus could mutate or you could have multiple strains with different infection and death rates to mess up your models - not unlikely for a corona virus.
This is the country that threw away billions on computer systems for NHS.
We have that degree of fidelity?
Plus the virus could mutate or you could have multiple strains with different infection and death rates to mess up your models - not unlikely for a corona virus.
This is the country that threw away billions on computer systems for NHS.
We have that degree of fidelity?
H59/70
If you do get through this period and manage to infect all the low risk, then theoretically you can throw open the doors and let the elderly see the sun again. Herd immunity will protect the elderly even if a few stragglers still have the virus
...or it completely fails
If you do get through this period and manage to infect all the low risk, then theoretically you can throw open the doors and let the elderly see the sun again. Herd immunity will protect the elderly even if a few stragglers still have the virus
...or it completely fails
H60/70
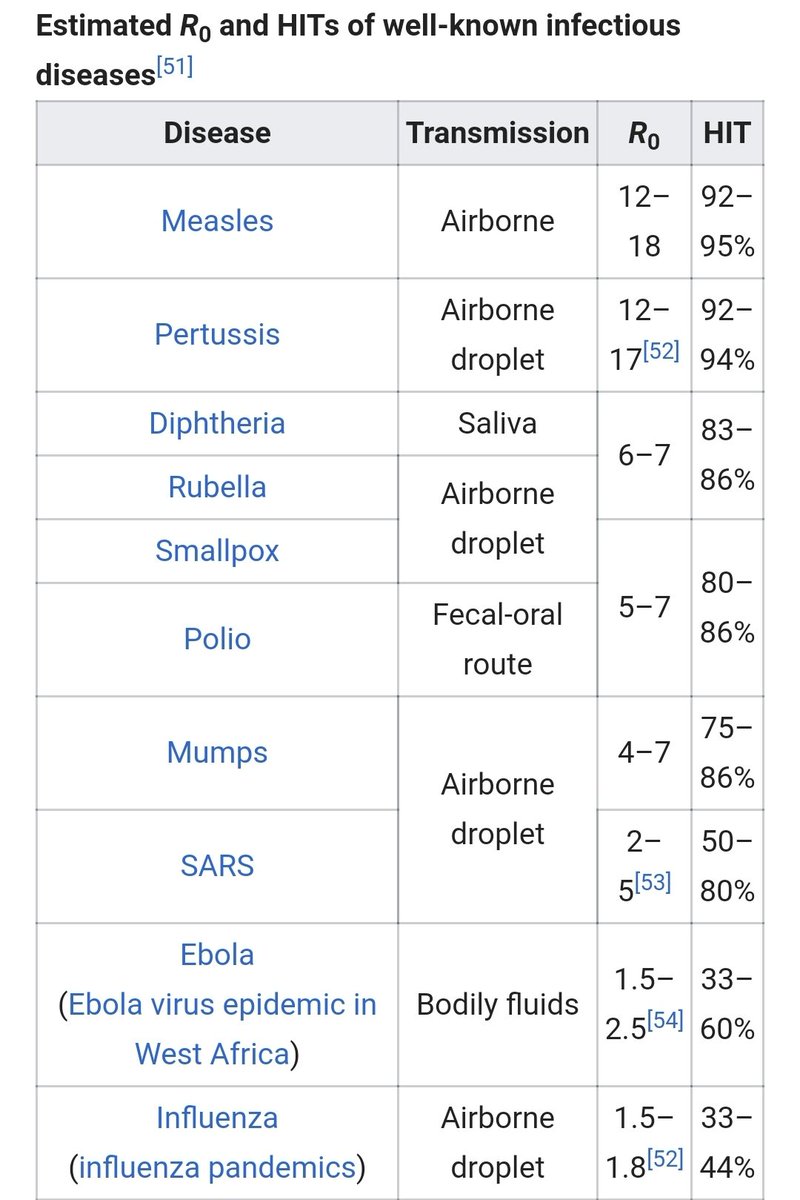
You see Herd Immunity despite Vallance waving his hand at 60%, is a very variable thing. That's why I gave a list of diseases that Humans have never managed to create immunity for at the start of this thread.
Let's look at these numbers closer⏬
You see Herd Immunity despite Vallance waving his hand at 60%, is a very variable thing. That's why I gave a list of diseases that Humans have never managed to create immunity for at the start of this thread.
Let's look at these numbers closer⏬
H61/70
You can see the significant variance. Moreover predicting corona viruses isn't easy due to variability:
We know it won't be flu at the bottom of the scale.
It probably won't be a 95% virus
It's in the middle - say SARS 50-80%.
Moreover, until you try, you don't know.
You can see the significant variance. Moreover predicting corona viruses isn't easy due to variability:
We know it won't be flu at the bottom of the scale.
It probably won't be a 95% virus
It's in the middle - say SARS 50-80%.
Moreover, until you try, you don't know.
H62/70
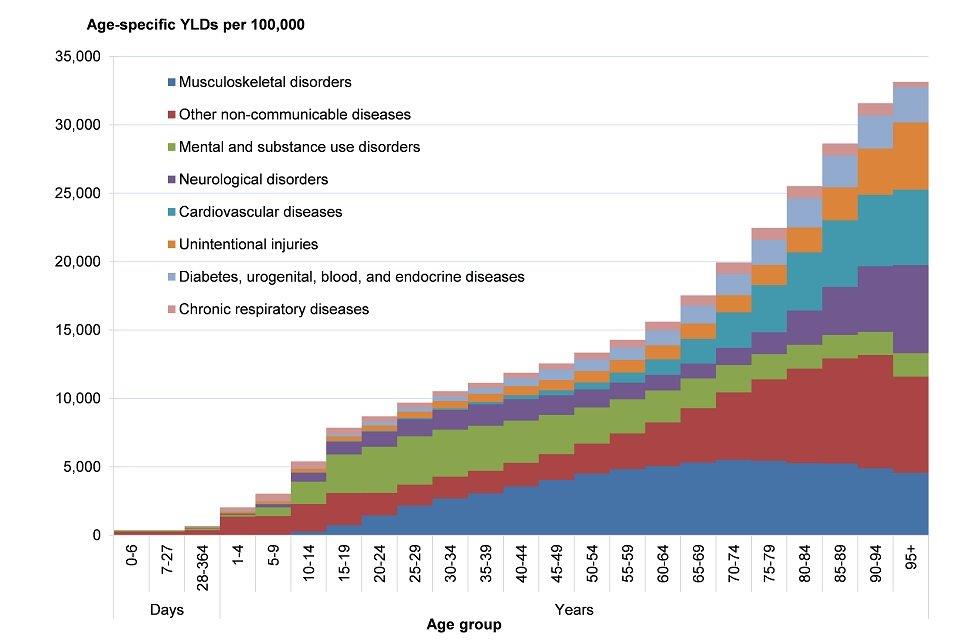
The over 60s are where covid deaths start to spike, so let's assume that's high risk.
Plus chronic disease (below) under 60
Plus has anyone considered carers? Who presumably need to stay unexposed.
Either way I get to ~30% +/-5% of the pop.
The over 60s are where covid deaths start to spike, so let's assume that's high risk.
Plus chronic disease (below) under 60
Plus has anyone considered carers? Who presumably need to stay unexposed.
Either way I get to ~30% +/-5% of the pop.
H63/70
So even if this were an exact science and it really isn't, if HI is at th high end of SARS, it will fail.
But we are not a demographically distributed society. So in some young areas you might have 80%.
What about Eastbourne?
So even if this were an exact science and it really isn't, if HI is at th high end of SARS, it will fail.
But we are not a demographically distributed society. So in some young areas you might have 80%.
What about Eastbourne?
H64/70
Then earlier I mentioned viral mutation. What if it mutates and half your low risk are no longer immune? We think btw covid19 has already mutated twice.
Or what if two strains occur?
I shudder to think about the validity of predictions on an unknown virus for 66m people
Then earlier I mentioned viral mutation. What if it mutates and half your low risk are no longer immune? We think btw covid19 has already mutated twice.
Or what if two strains occur?
I shudder to think about the validity of predictions on an unknown virus for 66m people
H65/70
Beyond that you have lack of compliance and God knows what coordination to make sure people leave home at the right stage. And if you need more time?
But the final problem is what you do if HI is, e.g. 70%.
Who's going to pull grandma from home to get the numbers up?
Beyond that you have lack of compliance and God knows what coordination to make sure people leave home at the right stage. And if you need more time?
But the final problem is what you do if HI is, e.g. 70%.
Who's going to pull grandma from home to get the numbers up?
H66/70
4.1 IS IT WORTH IT ANYWAY?
I think UKGov will argue that we should go through all this and if we fail, it'll be worth it anyway.
They'll have to given they deliberately sabotaged containment.
Unfortunately, the list of reasons for why that's false logic is long.
4.1 IS IT WORTH IT ANYWAY?
I think UKGov will argue that we should go through all this and if we fail, it'll be worth it anyway.
They'll have to given they deliberately sabotaged containment.
Unfortunately, the list of reasons for why that's false logic is long.
H67/70
But dear reader I'm sure others will eventually pick this up. So I'll only give you two.
A) You made it far worse.
You see the Government's upfront assumption is wrong. I don't know what they assumed, I said 80% to be cautious. It could be they thought a 100% rate.
But dear reader I'm sure others will eventually pick this up. So I'll only give you two.
A) You made it far worse.
You see the Government's upfront assumption is wrong. I don't know what they assumed, I said 80% to be cautious. It could be they thought a 100% rate.
68/70
By not containing covid it will be that
But what if we had followed WHO guidelines strictly? Best in class is below 50%.
Plus you have uncontained distribution of virus to contend with even with bellows. You could end up with higher than avg death rates for high risk.
By not containing covid it will be that
But what if we had followed WHO guidelines strictly? Best in class is below 50%.
Plus you have uncontained distribution of virus to contend with even with bellows. You could end up with higher than avg death rates for high risk.
69/70
If this were peas, it might not matter. But the swing I describe above is an additional 1.5% deaths in a population of 66m. That gives a number of extra deaths I don't want to write down.
The problem. The amount of confounding factors are huge, and the errors unthinkablee
If this were peas, it might not matter. But the swing I describe above is an additional 1.5% deaths in a population of 66m. That gives a number of extra deaths I don't want to write down.
The problem. The amount of confounding factors are huge, and the errors unthinkablee
70/70
2nd reason?
Hubris, Arrogance, Sociopathy
Ignore the world - strategy which is at best marginal for a disease you don't know?
Deliberately overexpose us?
So unprepared you have no guidance? Logistics?
No consultation?
That's not science
It's a crime against humanity.
2nd reason?
Hubris, Arrogance, Sociopathy
Ignore the world - strategy which is at best marginal for a disease you don't know?
Deliberately overexpose us?
So unprepared you have no guidance? Logistics?
No consultation?
That's not science
It's a crime against humanity.