1/important clarification from AL Med board- initiation of a controlled substance can be done without in-person exam for duration of this declared public health emergency. This partially alleviates pressure on long-term opioid recipients. I’ll clarify why “partially” next 

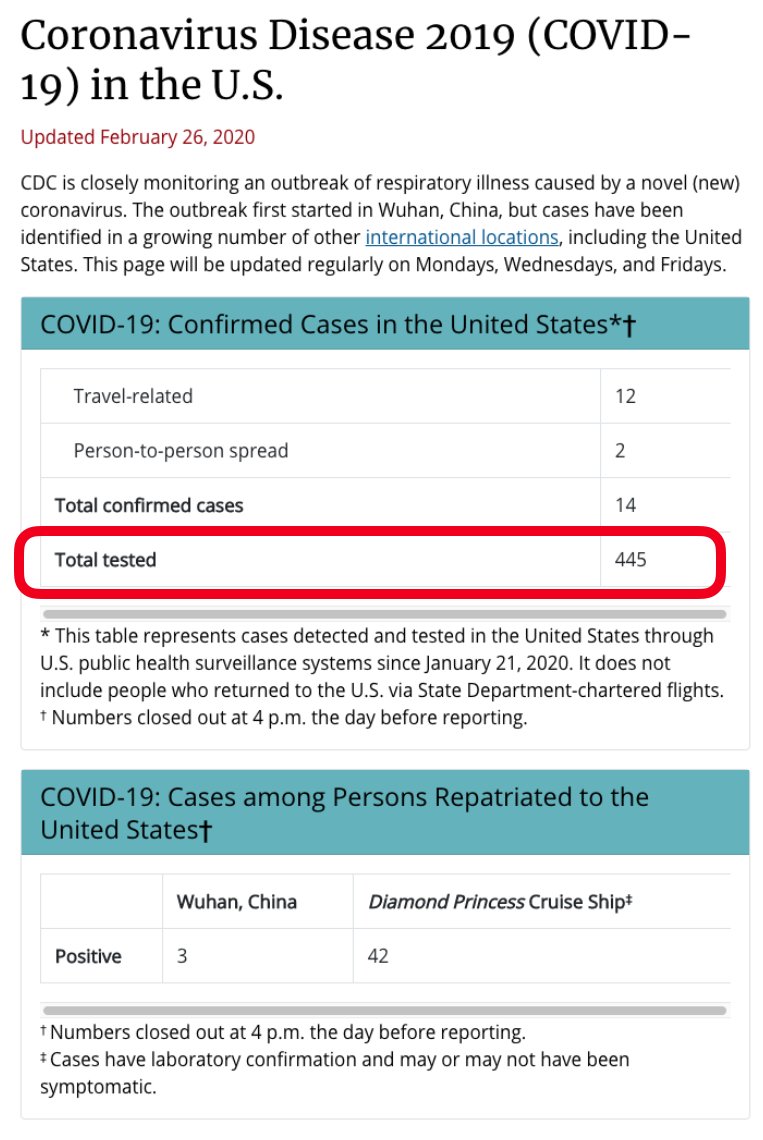
2/The public health issue is 10 mn pain patients on long term #opioids who must repeatedly see their docs in-person to CONTINUE the Rx’s. It is a major risk to them and the health system. Did DEA require that, ever? Not exactly, but in a way EVERY agency influencing opioids does!
3/Docs caring for patients on long term opioids have to guess how to continue the Rx without being subject to suspicion, investigation & rebuke from a variety of actors, including but not limited to law enforcement (quality metrics, insurers). ALL treat continuation as suspicious

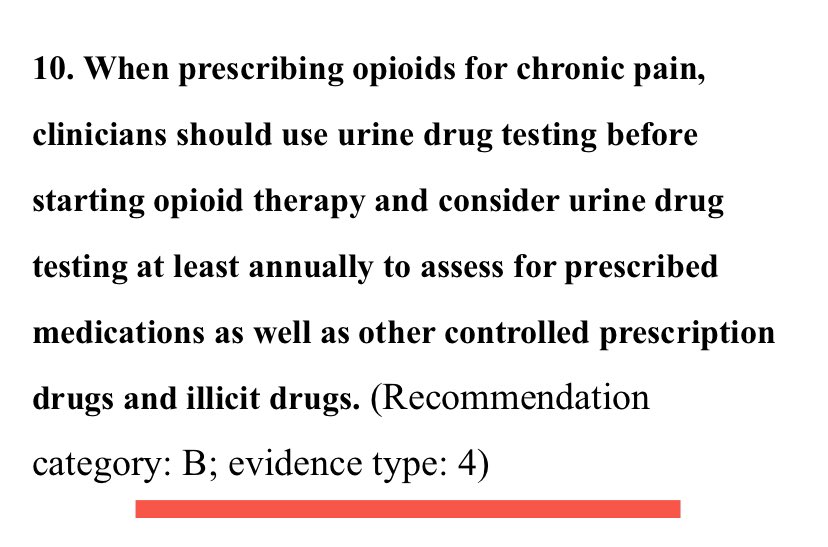
4/So to continue opioid Rx & remain “above reproach” clinicians are under pressure to document repeated evaluations, with urine drug tests. Many see the visit & urine test as a way to show the prescribing is “bona fide”. @CDCgov rec.. note “evidence type=4” means “horribly weak”
5/Was there a specific rule that docs MUST see the patient every month? Mostly not. There WAS a tacit q3 month rule from DEA. But mostly the reality is a collection of vectors that caused many MDs to end all long term opioid prescribing. Those who continue an Rx feel imperiled

6/So the default is to have disabled patients travel (long distances) to the last docs willing to shoulder a risk - some of are in fact “high risk” (alcohol use?coexisting mental illness?). But they should not be traveling to doc offices in a pandemic. And the urine tests?
7/I will say that urine testing is sometimes revelatory (patient doesn’t take the pills! Patient used cocaine!) but I am afraid we often use them poorly. And they don’t really assure a clinical practice is offering good pain care
8/What the temporary DEA& Board declarations imply (beyond reassurance re: initiation)is recognition that in a crisis, “we see the need to adjust what you do”. Ultimately however docs will consider their risks in light of all pressures. My TEDx on this:
9/If this pandemic doesn’t kill us, and I hope it doesn’t, it may also be a chance to recognize that good care on opioid continuation, with its clinical risk & benefit, is based more on detailed & careful clinical conversation, even by phone/telehealth