1/ It is very weird to have to interpret national policy exclusively through what's said in press briefings.
But I think the administration just announced a major shift in
#COVID19 strategy.
And I think I agree, with some caveats.
But I think the administration just announced a major shift in
#COVID19 strategy.
And I think I agree, with some caveats.
2/ Here's what I heard at the White House coronavirus task force holds news briefing today
(very weird not have @CDCgov Principal Deputy Director Ann Schuchat leading this effort tbh - read her bio- she was built in a lab for this) cdc.gov/about/leadersh…
(very weird not have @CDCgov Principal Deputy Director Ann Schuchat leading this effort tbh - read her bio- she was built in a lab for this) cdc.gov/about/leadersh…
3/ This ties into the desire to balance the impact on economy with control of the outbreak.
The approach is to use surveillance data to guide decision-making on where lockdowns can be relaxed, maintained, or intensified.
That's how this should have been done in the 1st place
The approach is to use surveillance data to guide decision-making on where lockdowns can be relaxed, maintained, or intensified.
That's how this should have been done in the 1st place
4/ As I suggested a lifetime ago it seems, we should have a clearly articulated plan, which involves having the right testing and surveillance data; and a clear algorithm for when to switch from containment to mitigation to suppression-and when to go back
5/ In the absence of the data, a strategy, and federal public health leadership, we kind of stumbled into lockdowns across the country. Businesses, schools, state and local officials began to act on their own, and at some point, it just became unstoppable.
But for how long?
But for how long?
6/ What's being proposed today is to identify "green areas" where it's safe to lift lockdowns, and where it's not
As Dr Birx began, she said there are low # cases (<200) in 19/50 states- almost 40% of the country, despite what she characterized as adequate testing. (Key Q!)
As Dr Birx began, she said there are low # cases (<200) in 19/50 states- almost 40% of the country, despite what she characterized as adequate testing. (Key Q!)
7/ Do we have adequate public health capacity in those 19 states? She mentioned need for ongoing social distancing & continued containment- in particular traditional public health strategies (active case finding, contact tracing, isolation, and quarantine)
Let's make sure we do
Let's make sure we do
8/ My worry is whether we'll have a false sense of security (absence of evidence <> evidence of absence)- will we allow outbreaks in Wichita Kansas & Little Rock, Arkansas to flare if we don't have strong systematic surveillance?
Puts a lot of pressure on frontline docs & PH
Puts a lot of pressure on frontline docs & PH
9/ The other part was to draw a red line around the current hotspots- and to presumably intensify suppression and shift resources (including vents, PPE, people) to those areas.
She mentioned NY metro, Wayne County MI, Cook County Chicago, New Orleans. All dense urban areas.
She mentioned NY metro, Wayne County MI, Cook County Chicago, New Orleans. All dense urban areas.
10/ She didn't mention it specifically, but that leaves a lot of the country in between, including where I'm sitting now in Maryland
What here? I think we need to maintain lockdowns in these areas with brewing epidemics until we see strong evidence of outbreak curve flattening
What here? I think we need to maintain lockdowns in these areas with brewing epidemics until we see strong evidence of outbreak curve flattening
11/ it was a small wonky detail, but she also talked about allocating high capacity (96 well) vs low capacity (4-8 well) lab testing machines based on the outbreak profile of different areas
But this requires knowing not just where it's hot now, but also "where it's moving next"
But this requires knowing not just where it's hot now, but also "where it's moving next"
12/ This makes all the sense in the world, but let's be clear, would be a huge lift for a response that up until now, has not given much confidence in getting testing in the field, much less getting systematic adequate sampling, conjoined clinical and onset information, exposures
13/ I've heard about conversations in the field in past week - from labs approached by DHS folks, to EHR vendors, Hospital associations, public health authorities, seemingly part of a concerted effort to get the surveillance ship in order, stymied by lack of institutional memory
14/ I wish the CDC was clearly in the drivers seat here.
THEY DO SURVEILLANCE.
I really don't understand what is happening there, but I am willing to be hopeful that we can get a stronger federal hand guiding state/local decision making.
THEY DO SURVEILLANCE.
I really don't understand what is happening there, but I am willing to be hopeful that we can get a stronger federal hand guiding state/local decision making.
15/ Dr Birx mentioned CDC having 2 major roles
A) helping state/locals with intense contact tracing- including providing workforce for counties that move into containment
B) Conducting a serosurvey to understand true rate of underlying infections
(I did both when I was at CDC)
A) helping state/locals with intense contact tracing- including providing workforce for counties that move into containment
B) Conducting a serosurvey to understand true rate of underlying infections
(I did both when I was at CDC)

16/ A serosurvey is somewhat distinct from this new strategy, but long overdue
Modelers have told us that the most important input variable they don't have is the infection prevalence-it literally changes model outputs from whether this ends up like the 1918 flu pandemic-or 1957
Modelers have told us that the most important input variable they don't have is the infection prevalence-it literally changes model outputs from whether this ends up like the 1918 flu pandemic-or 1957
17/ She alluded to @neil_ferguson testimony that outbreak could kill 20k in UK vs 500k as depending on this factor
I see some wishful thinking on this. Neil has clarified he meant WITH continued suppression
But it's a real question. If 30% of pop in Brooklyn already has it 🥳
I see some wishful thinking on this. Neil has clarified he meant WITH continued suppression
But it's a real question. If 30% of pop in Brooklyn already has it 🥳
18/ [sidebar] I'm somewhat optimistic in recent days even countries like Iran that have not - to my knowledge- implemented very successful suppression or contact tracing have begun to see a flattening of the curve on deaths.
it could be (more) under-reporting, or herd immunity?
it could be (more) under-reporting, or herd immunity?

19/ Back to Dr Birx- who raised the question of why the attack rate is rarely seen higher than 1:1000 population except for Monaco and Lichtenstein (to be fair, also Brooklyn and Queens, I think- @bijans has been keeping track. )
Maybe this outbreak isn't going to be so bad?
Maybe this outbreak isn't going to be so bad?
20/ All this seems to be laying the groundwork for lifting lockdowns in significant (more rural) parts of the country.
But will we know if things start to go off the rails?
This is where she brought in (though she didn't name it exactly) - the syndromic surveillance platform
But will we know if things start to go off the rails?
This is where she brought in (though she didn't name it exactly) - the syndromic surveillance platform
21/ I talked about this already- can read my string there (and will probably be explaining more about it in days to come I think!)
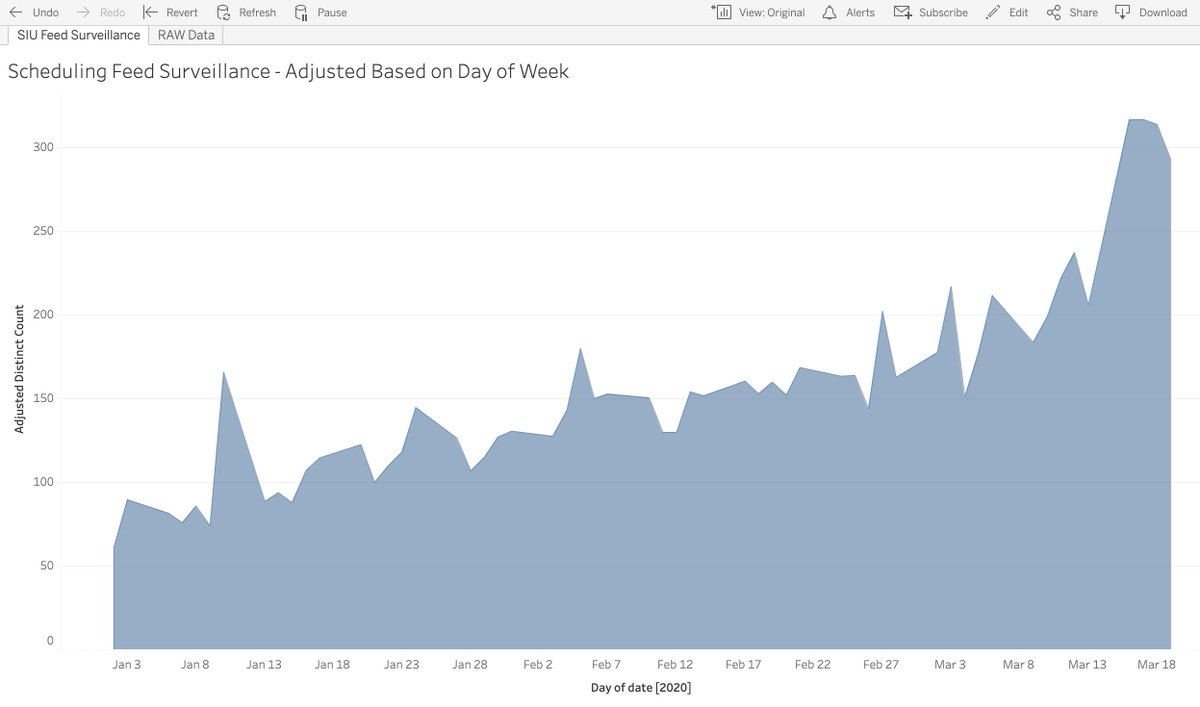
22/ As she explained it we have hospitals emergency rooms reporting Influenza-like illness to state/local health departments (actually just shipping over de-identified registration logs for them to analyze and classify into syndromes)- and you can use that to detect COVID
23/ To be clear, you need a pretty big signal. Like ~ 50 cases of cough/fever in one day for a big city.
that means hundreds of symptomatic cases, and clearly widespread community transmission.
it's a safety net for sure, but not a substitute for systematic lab surveillance
that means hundreds of symptomatic cases, and clearly widespread community transmission.
it's a safety net for sure, but not a substitute for systematic lab surveillance
24/ You can probably increase the sensitivity of detection of COVID if you can get a gold standard from NYC or Seattle, and use it to fine-tune the syndrome definition (add "Change in Taste" remove "Sore Throat"?), look for relative paucity of increase in youngest age group...
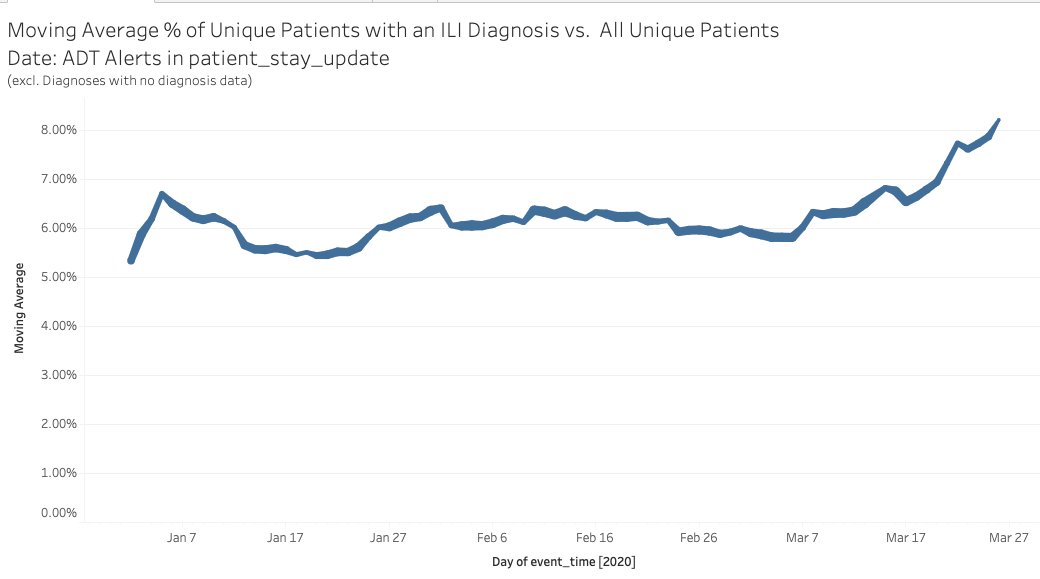
25/ I think the folks in CDC have probably done this, but it would be good for them to share that with everyone who has access to utilization data in healthcare- including health plans and provider groups like ours
@AledadeACO supports 550 practices in 27 states-here's our trend
@AledadeACO supports 550 practices in 27 states-here's our trend
26/ But the strangest part of this strategy is going to be managing the introduction of "sparks" from the hot zones to the green zones. I hope that we don't trample our civil society and rely instead on massively upgraded education and public health workforce / contact tracing
27/ When asked Dr Birx said "we need highly responsible behavior" when people move between counties, they should take "appropriate precautions" as they move between places
But if schools/ work/ restaurants are closed in one county, and open in an adjoining one- would you move?
But if schools/ work/ restaurants are closed in one county, and open in an adjoining one- would you move?
...and then to see that #VaguelyExplainSomething is trending