,
25 tweets,
6 min read
Read on Twitter
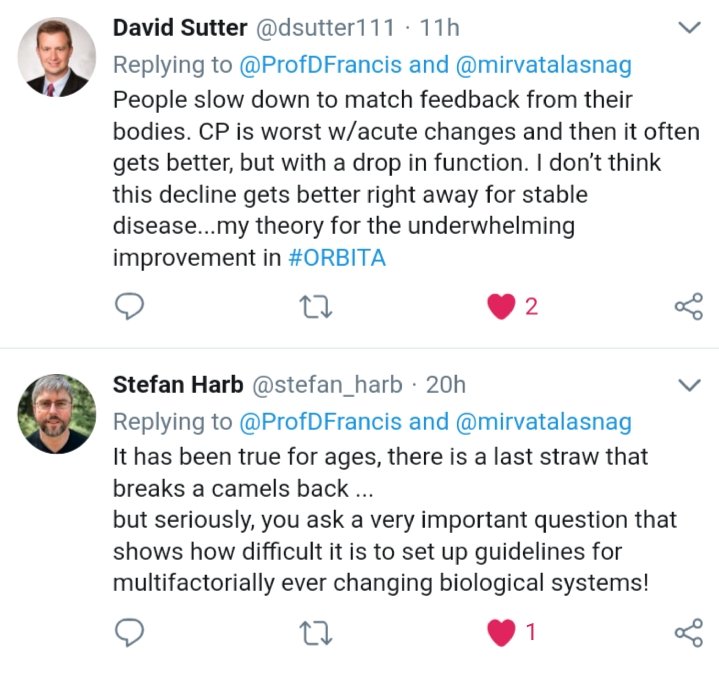
Think about what this means!
Many patients with STEMI have impressive underlying disease, either extensive atheroma in the index vessel or tight stenosis in other vessels too.
Before today's thrombus, how were they walking around asymptomatic ?
Thought provoking suggestions!
Many patients with STEMI have impressive underlying disease, either extensive atheroma in the index vessel or tight stenosis in other vessels too.
Before today's thrombus, how were they walking around asymptomatic ?
Thought provoking suggestions!
Or ...
Perhaps much of what we call "ischemia", for lack of a better word, is asymptomatic.
If true, it would have several effects.
Perhaps much of what we call "ischemia", for lack of a better word, is asymptomatic.
If true, it would have several effects.
1. A sizeable proportion of STABLE ischemic heart disease patients, the first time they seek medical help is when they have advanced (e.g. v tight, or 2 or 3 vessel) disease.
Do you see this in your practice ?
Do you see this in your practice ?
2. The day before they felt symptoms, the state of their arteries was almost the same and yet they were:
In a separate strand now please think about people with symptoms in the chest area, and turn out to have normal arteries.
3. What do we do with such patients ?
3. What do we do with such patients ?
Let's think about how common the above situation is.
Look at Manesh Patel's NEJM paper.
Look at Manesh Patel's NEJM paper.
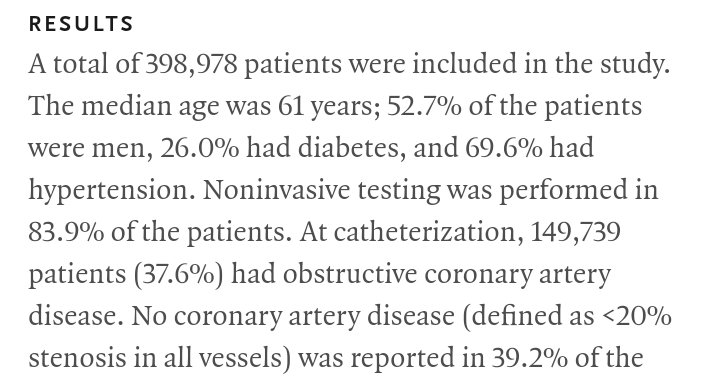
It focussed on patients having angiography for first diagnosis of coronary disease and without major valve problems, previous CABG or PCI etc.
First timers.
How many patients, roughly ?
First timers.
How many patients, roughly ?
About what proportion had unobstructed arteries?
(They defined this as nothing >50% in LMS and nothing >70% in the other main arteries)
(They defined this as nothing >50% in LMS and nothing >70% in the other main arteries)
So, on the one hand, there is a substantial proportion of people with bad coronary disease who have no awareness of it.
And on the other hand we a substantial proportion of people with symptoms etc and no obstructive coronary disease.
And on the other hand we a substantial proportion of people with symptoms etc and no obstructive coronary disease.
In light of this, when a patient has chest pain, and they go through to have angiography and are found to have severe coronary disease, is it SCIENTIFICALLY RELIABLE to assume that the CHEST PAIN is caused by the CORONARY STENOSIS?
Correct answer to the _previous_ question:
60% Unobstructed arteries (no lesion more than 50% in LMS or 70% elsewhere)
including
40% NORMAL arteries (no lesion more than 20%)
60% Unobstructed arteries (no lesion more than 50% in LMS or 70% elsewhere)
including
40% NORMAL arteries (no lesion more than 20%)
Our clinical practice when we see someone with plausible symptoms + tight coronary artery disease is that we ASSUME that the coronary disease is the cause of the symptoms.
This is what we normally do.
This is what we normally do.
Does "normally doing a thing", cause people doing it to think that that particular "thing" makes sense to do?
If in doubt, think about:
Bullfighting in Spain
Seal-clubbing in Canada
Gun-carrying in USA
If in doubt, think about:
Bullfighting in Spain
Seal-clubbing in Canada
Gun-carrying in USA
If you thought like this, and you were designing a placebo-controlled trial of PCI to relieve symptoms, and randomized symptomatic patients with tight disease, 94-96% of them having 1 or more positive ischemia tests, what would you have expected the effect of PCI to be?
Plain old Balloon Angioplasty gives +96s exercise time [ACME trial, NEJM 1992].
Before reading ORBITA, what benefit would you have expected for patients having not POBA but modern stenting. 94-96% of them had 1 or more ischemia tests.
Before reading ORBITA, what benefit would you have expected for patients having not POBA but modern stenting. 94-96% of them had 1 or more ischemia tests.
The clinical assumption is that when we see
Symptoms + Positive ischemia test + Severe coronary lesions(s)
we assume the causation is obvious:
STENOSIS -> ISCHEMIA -> SYMPTOMS
If this assumption is CORRECT, what would you expect to be the symptomatic effect of stenting lesions?
Symptoms + Positive ischemia test + Severe coronary lesions(s)
we assume the causation is obvious:
STENOSIS -> ISCHEMIA -> SYMPTOMS
If this assumption is CORRECT, what would you expect to be the symptomatic effect of stenting lesions?
If the assumption is INCORRECT, what will the blinded effect of PCI on symptoms be?
(i.e. if much of symptoms in pts with coronary disease is NOT due to coronary disease, and much of coronary disease does NOT cause symptoms, how effective will PCI be in relieving symptoms?)
(i.e. if much of symptoms in pts with coronary disease is NOT due to coronary disease, and much of coronary disease does NOT cause symptoms, how effective will PCI be in relieving symptoms?)
The results of ORBITA were indeed disappointing to @rallamee and me.
Below is a still image of Justin Davies, Rasha and myself from the live video feed at ORBITA hq when the results emerged.
Rasha is pointing to the +16.0 saying "maybe that is a fly, not a decimal point ?"
Below is a still image of Justin Davies, Rasha and myself from the live video feed at ORBITA hq when the results emerged.
Rasha is pointing to the +16.0 saying "maybe that is a fly, not a decimal point ?"

Now let's re look at the +96 s unblinded POBA at 6 months (plenty of time for restenosis) in ACME, 200pts.
and the +16s blinded stenting (94 to 96% with 1 or more positive ischemia tests) at 6 weeks in ORBITA, 200pts.
Most plausible explanation for difference?
and the +16s blinded stenting (94 to 96% with 1 or more positive ischemia tests) at 6 weeks in ORBITA, 200pts.
Most plausible explanation for difference?
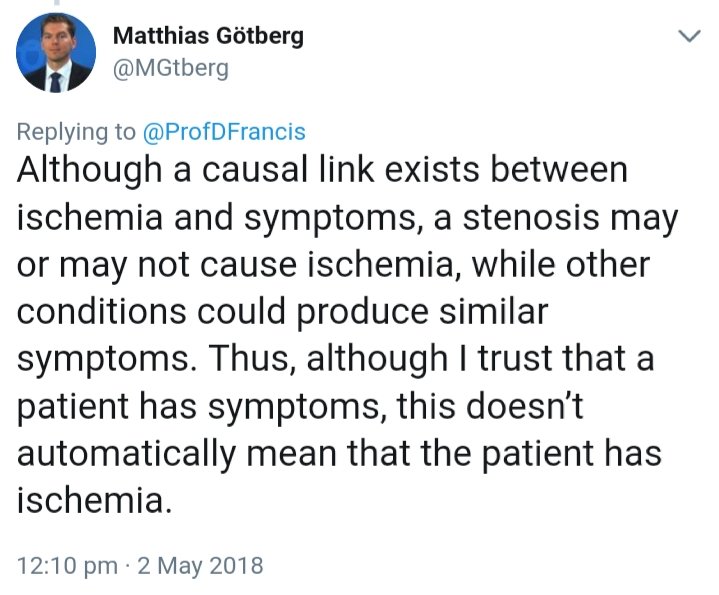
Matthias' point is perfectly correct.
But the challenge here is not whether there is ischemia in ORBITA: 94 to 96% of patients had 1 or more positive ischemia tests. So answer = yes.
The challenge is whether their plausibly ischemic symptoms did in fact arise from ischemia.
But the challenge here is not whether there is ischemia in ORBITA: 94 to 96% of patients had 1 or more positive ischemia tests. So answer = yes.
The challenge is whether their plausibly ischemic symptoms did in fact arise from ischemia.
Blinded studies don't have the advantage of Faith Healing, which is an important part of the therapeutic effect of PCI.
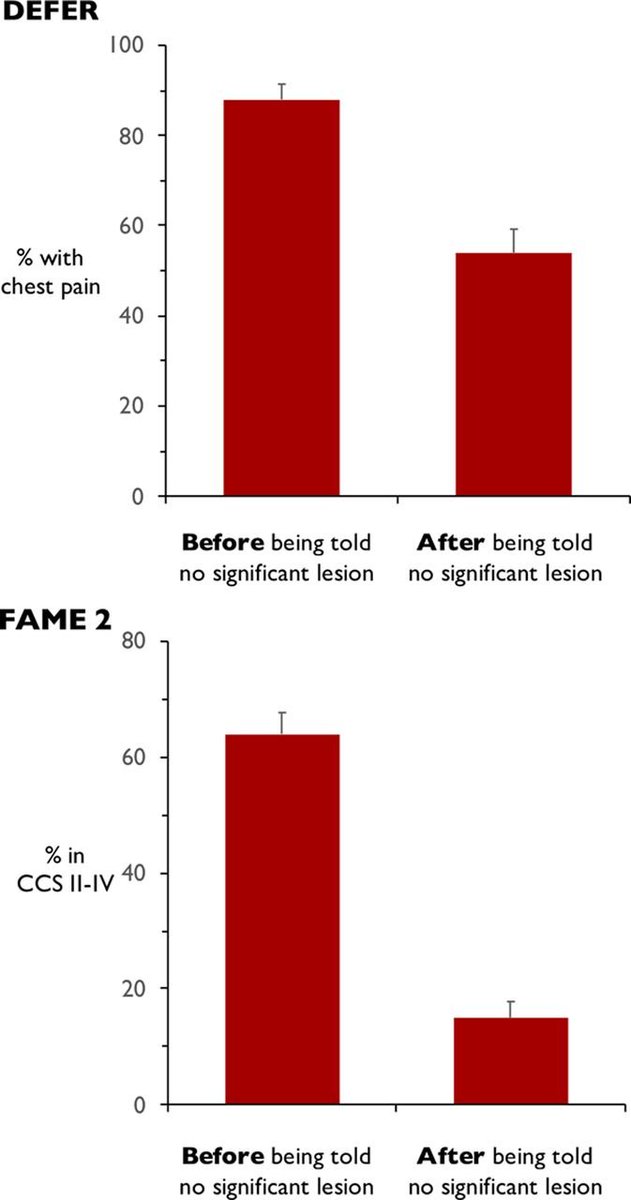
circoutcomes.ahajournals.org/content/11/3/e…
Here is the effect of Faith Healing ALONE, no POBA, no stenting. Powerful stuff, by any yardstick!
circoutcomes.ahajournals.org/content/11/3/e…
Here is the effect of Faith Healing ALONE, no POBA, no stenting. Powerful stuff, by any yardstick!
Well well.
We have a candidate for dangerous doctor of the year.
Yup. I am arguing against the existence of even a conceptual gold standard for "ischemia".
We have a candidate for dangerous doctor of the year.
Yup. I am arguing against the existence of even a conceptual gold standard for "ischemia".
As dangerously disrespectful @nsivcd Chris Cook says, why should you and I have the same threshold of flow reduction to have chest pain?
And even if, by some fluke, we have the same threshold of flow to give us both pain, why should we have the same threshold to get stress echo wall motion abnormality ?