[THREAD] Our tips on small bore chest tube placement for pleural effusion! Performed by a resident @BostonCityEM supervised by fellows @BUPulmonary. We'd love your input! Not a comprehensive guide. Made with written patient authorization. #meded #FOAMcc #pulmcc 
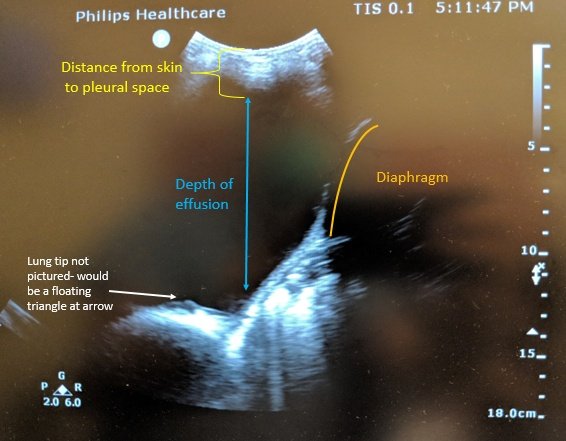
For new large unilateral effusions such as this, we place a chest tube if fluid pH <7.2, glucose <60. Without fluid studies, we place a tube empirically if effusion is large, loculated, infected, or likely to reaccumulate- except CHF/fluid overload.

First step: ultrasound. We position the probe with marker to the head, as lateral as possible. Intercostals tend to sag as you move towards the midline, so you could hit them when going above the rib. Lateral access is safest.
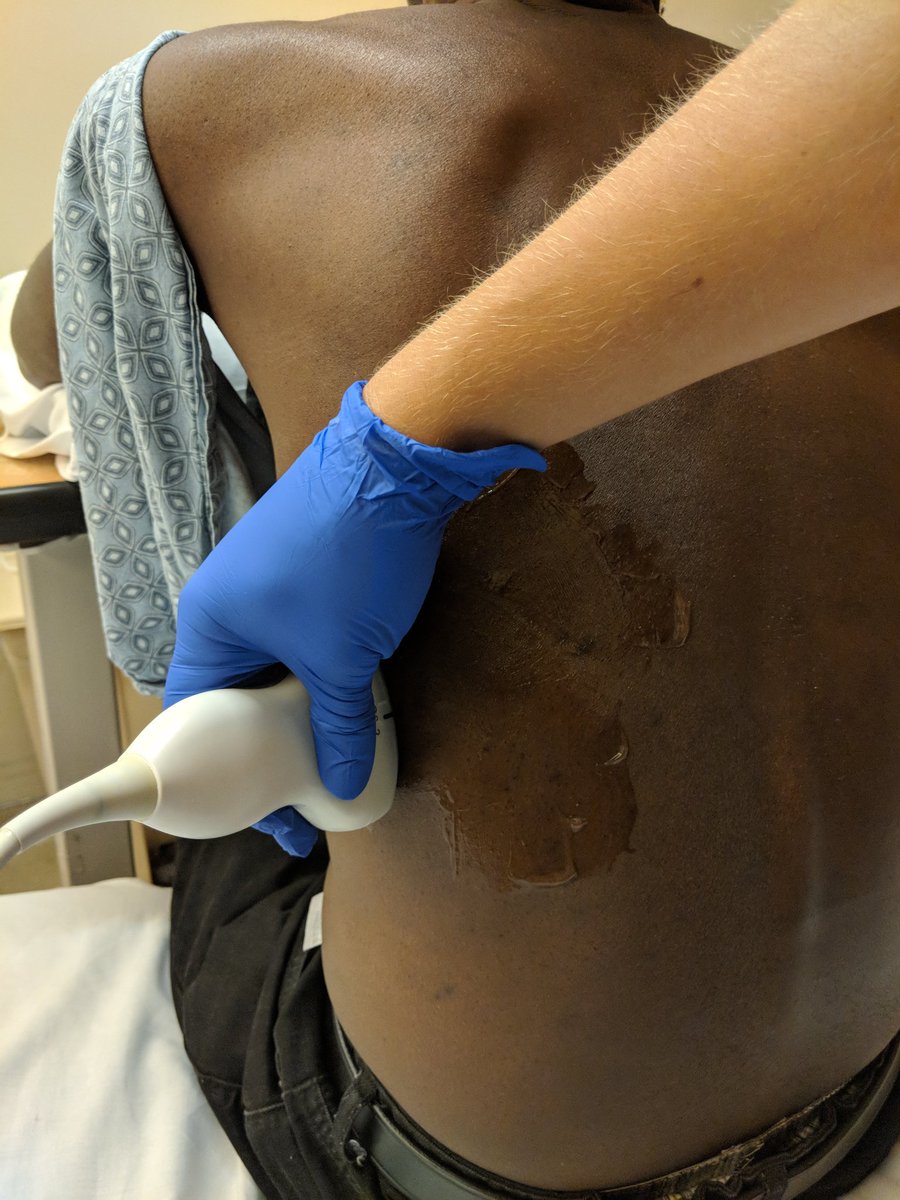
You've confirmed there is an accessible pocket. Next, set up the room. Have the patient sit up at the edge of the bed & lean forward onto a raised table. Ensure bed & table immobile. We will use the bed to set up our sterile field & equipment.
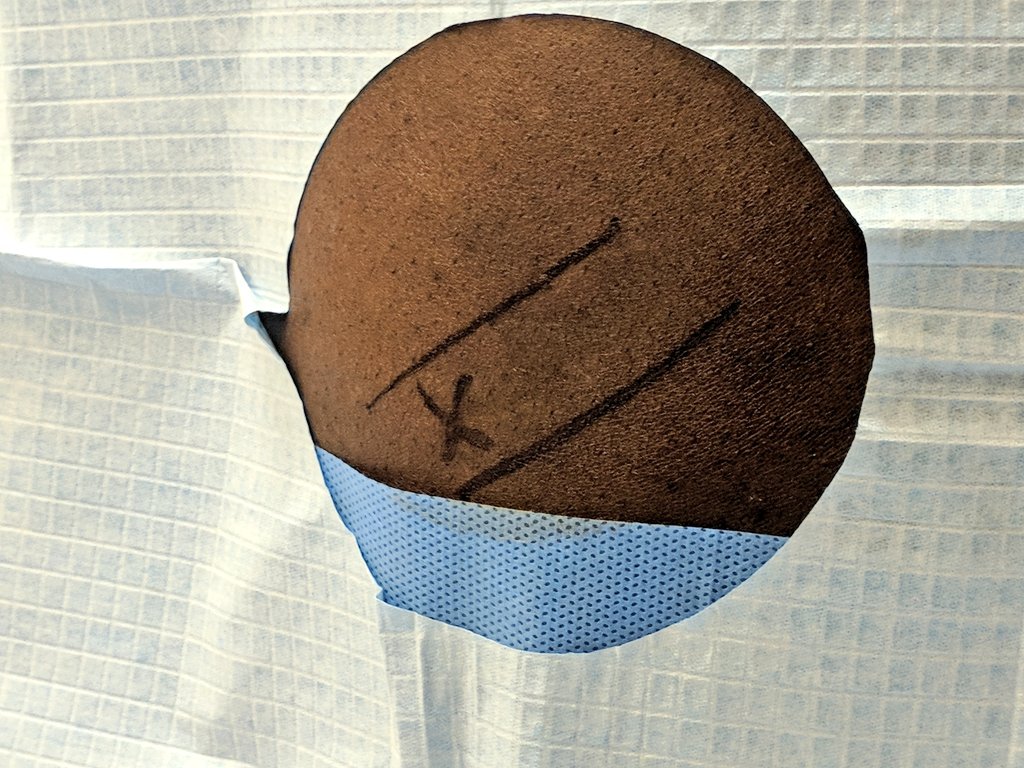
Now that the patient is positioned, confirm your ultrasound image again. Feel for the rib and have a good sense of the rib borders - you will need these landmarks. Mark the ribs and your site with ink and indentation so they persist after swabbing. Patient needs to be still now.
Prep is everything! Place a chux underneath the patient & set up sterile field. We use chlorhex swabs x3 on site & open equipment on the bed, using included towels & drapes to set up a large field. Repeat US if needed before swabbing. After swabbing, outline rib borders again.
The patient shouldn't move much now-- it could change your access point & increase risk. Consider using live/direct ultrasound if you're worried about fidgeting. For that, you'll need a sterile probe cover and probably an assistant.
Live/direct US not necessary for most tubes.
Live/direct US not necessary for most tubes.
Local anesthesia is critical. Start with small gauge needle, create wheal over the rib. Advance through wheal, attempt to hit rib. Switch to longer needle, feel and lido the rib.
Remember to tell the patient before every stick.
Remember to tell the patient before every stick.
We use the "walk up the rib" method to go just over the rib. When you feel bone, keep the needle perpendicular to rib, withdraw slightly, keep needle straight & elevate syringe & needle. Take small "steps" up until just over rib, then advance - always under negative pressure.
Ideally you have now created a wheal, anesthetized the periosteum liberally, created and anesthetized a track over the rib, ultimately applying lidocaine all the way up to the pleura. Doing this well is critical! We use 1% lido with or without epi.
Next, use a blade to make an incision. Keep it parallel with the rib, close to the center where you felt it. Your incision just needs to get through the skin to prepare for your needle & ultimately tube.
Others may prefer to nick after wire placement, this is just my preference.
Others may prefer to nick after wire placement, this is just my preference.
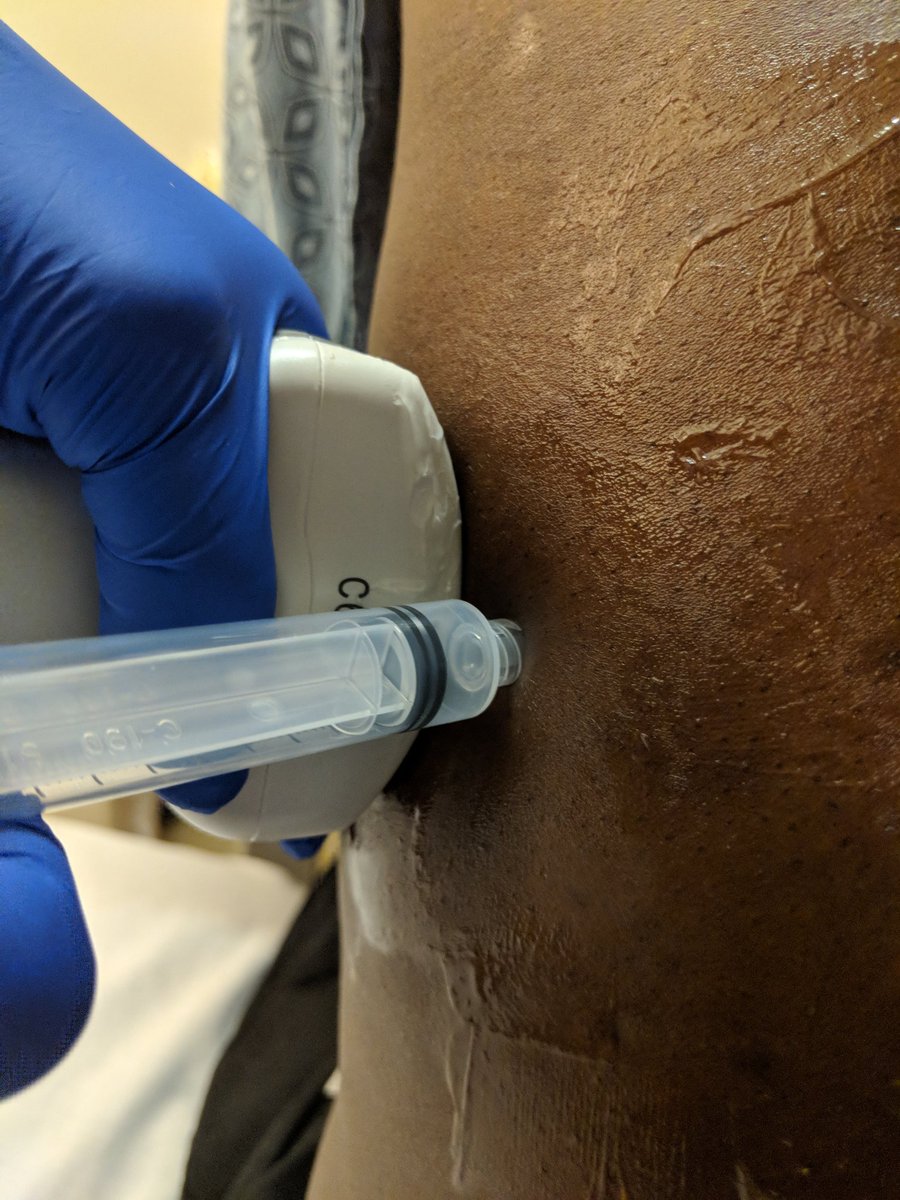
Now prepare your syringe-needle system and insert through your nick. You should definitely probe to the rib here, and lidocaine should ensure comfort. Once you hit the rib, "walk up" with very small steps until you go just over rib. Advance to pleural space.
Once you have access (fluid in syringe) you'll remove the syringe, keeping needle in place. Cover needle with thumb to minimize entrapped air. Insert wire into needle and angle needle down to guide wire to the base of the chest. Remove needle.
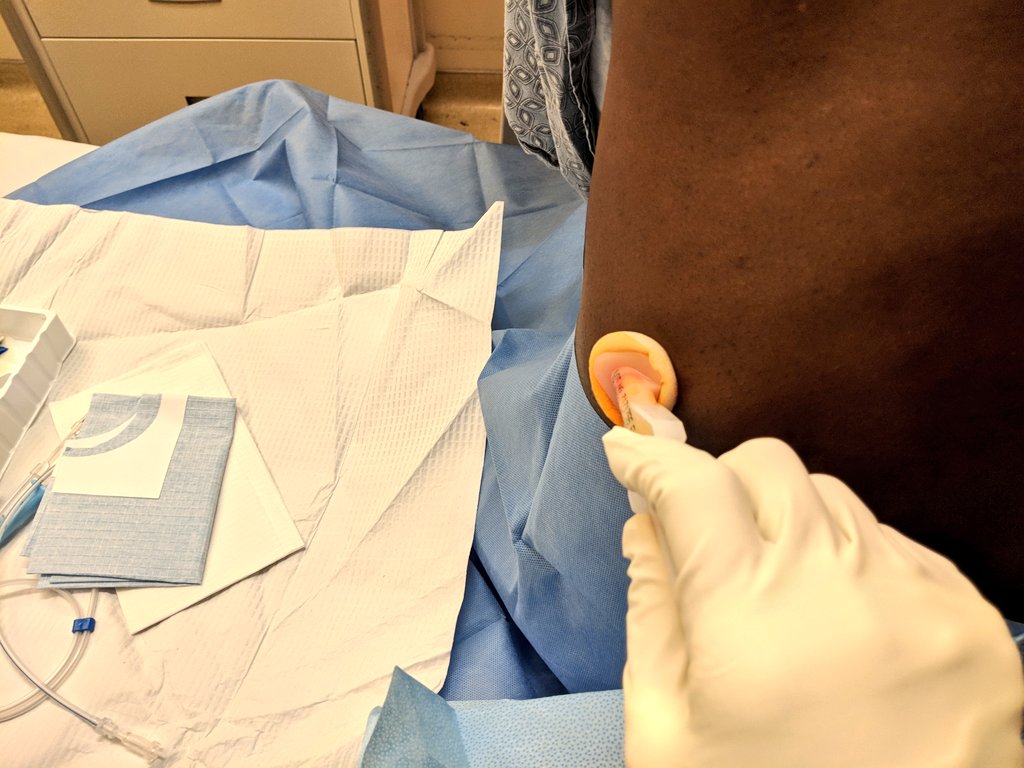
With wire in place, advance dilator to skin. Warn patient about this as you’ll be exerting pressure- it may be uncomfortable. As always, insert with twisting motion, hand close to skin. May need multiple dilators depending on tube size. Ensure dilator is hubbed & rotates easily.
Remove dilator, holding gauze as fluid may spurt out- good thing you have chux under pt, full PPE w/ face mask & shoe covers! With dilator out of the body, hold wire in place & rapidly pull dilator off the wire, thread tube over wire and insert into the pleural space to ~12cm.
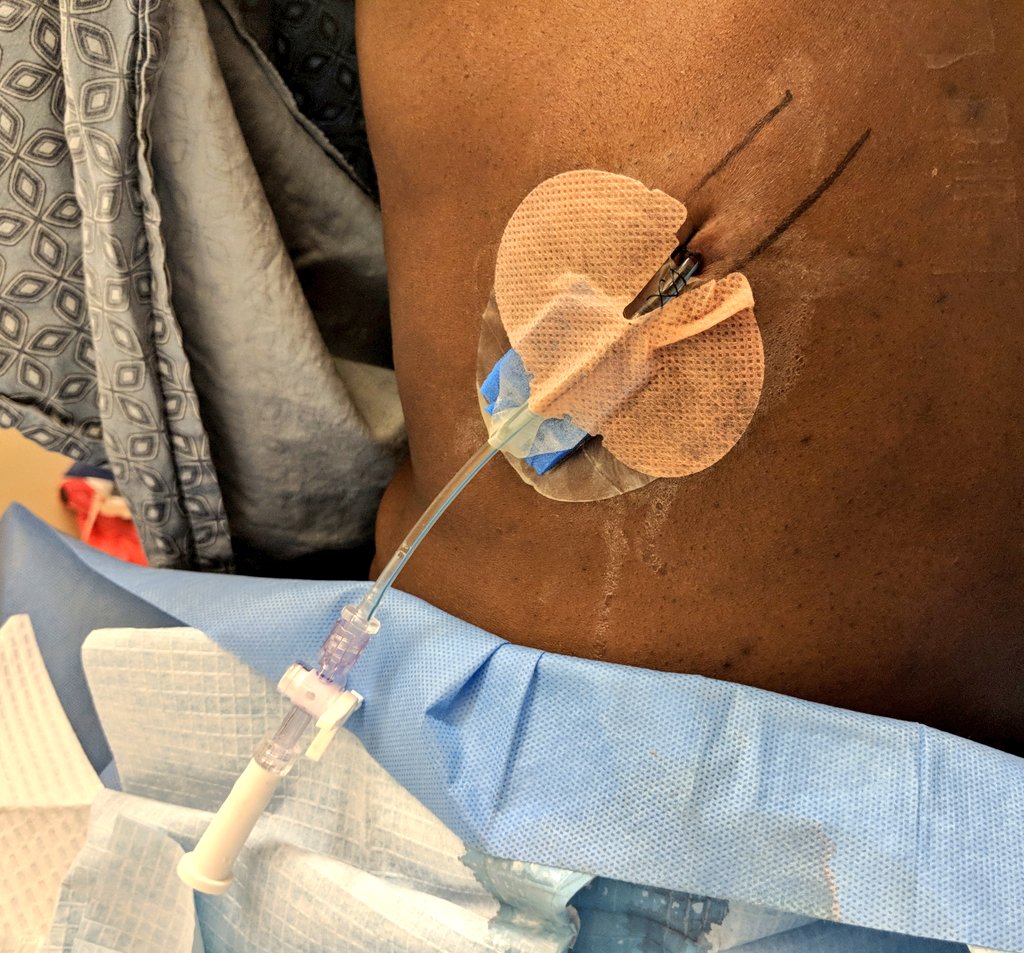
Our tubes have an inner stiffener. Holding the tube up to reduce the chance of introducing air, we remove the stiffener and wire simultaneously & promptly (as above). Attach a three way stopcock (as below). Take care now - - the tube is not secured and could easily slide out.
Next up: suturing the tube down. Start with a single anchor stitch, then braid around the tube. Some say it is better to braid along the length, others bunch the stitches. Regardless, stitches are not that effective- tube can & will slide right out without a secure dressing.
The dressing is critical. Use gauze to ensure a clean/dry site before attempting any dressing. A wet dressing is useless, and the dressing is what really holds the tube in place. We secure it to the front for patient comfort & use a few tegaderms to make it as secure as possible.


The tube is in and secure. Next, obtain your samples. Sterilize the vials and inoculate cultures at bedside for increased yield: ncbi.nlm.nih.gov/m/pubmed/21459…
And of course safe sample management is critical. Needlesticks happen right now!
And of course safe sample management is critical. Needlesticks happen right now!
Can't overstate the importance of technique with sample management. You need these micro studies to be excellent, so clean everything. Avoid needlesticks by avoiding bare needles. Use the holder device shown below!
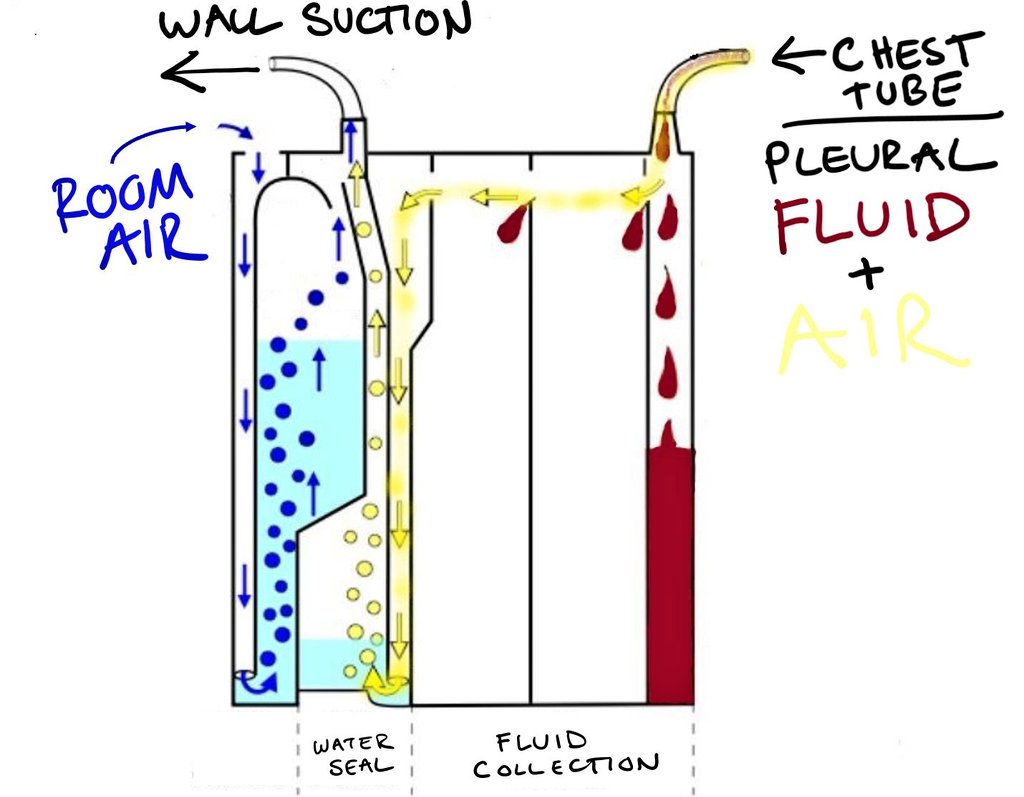
Next, hook the tube up to the box. We use @AtriumMedical Oasis, a "dry" system with a water seal. Confusing! See diagram below, ask questions!
FYI: clamp the system using the stopcock on the tube or using the sliding clamp over the drainage to the box.
FYI: clamp the system using the stopcock on the tube or using the sliding clamp over the drainage to the box.
Watch water level closely, have pt take breaths/cough. Bubbles= air leaking out of pt, into tube.
- flush tubes BID w/ stopcock
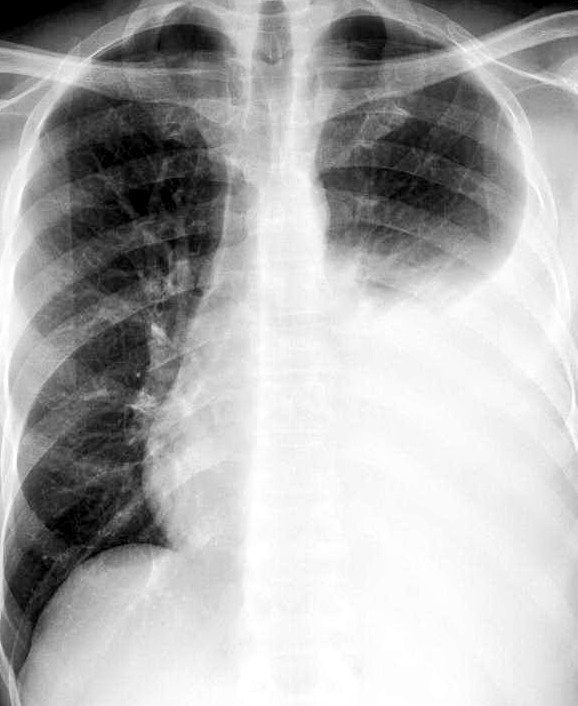
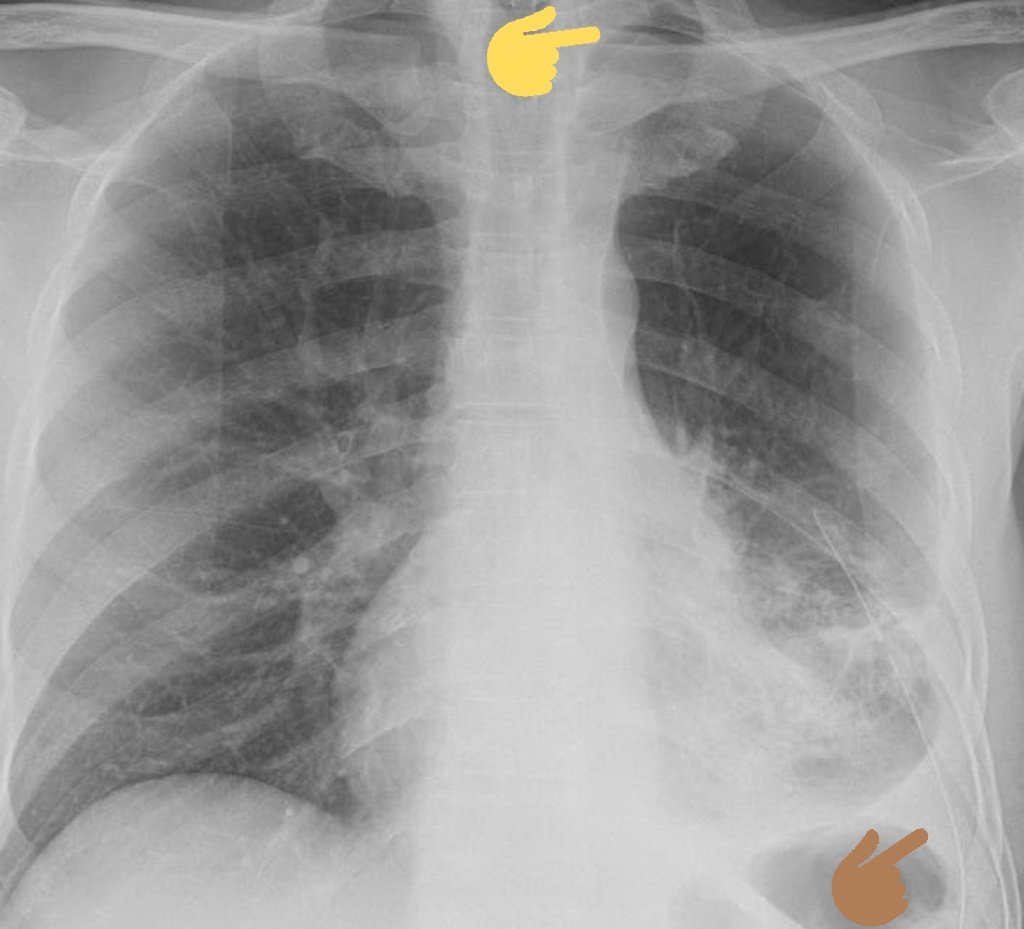
- always get a CXR. Air in pleural space: entrained during placement or pneumothorax? Repeat film later to confirm resolution.
Brown= tube, yellow= air
- flush tubes BID w/ stopcock
- always get a CXR. Air in pleural space: entrained during placement or pneumothorax? Repeat film later to confirm resolution.
Brown= tube, yellow= air
Hope you enjoyed this thread! Looking forward to hearing your tips and experiences in the comments.
If you're interested please check out our thread on central line insertion below!
If you're interested please check out our thread on central line insertion below!