,
16 tweets,
4 min read
Read on Twitter
1/
Why do we use urine antigen tests to diagnose respiratory pathogens?
Patients admitted with pneumonia are often diagnosed with S pneumoniae or legionella based on a positive URINE test.
Let's try and figure out why we search the urine to identify lung pathogens.
Why do we use urine antigen tests to diagnose respiratory pathogens?
Patients admitted with pneumonia are often diagnosed with S pneumoniae or legionella based on a positive URINE test.
Let's try and figure out why we search the urine to identify lung pathogens.

2/
First, a question: why are urine antigen tests often used to diagnose apparently non-urinary infections?
[NS = nephrotic syndrome; SC = sieving coefficient]
First, a question: why are urine antigen tests often used to diagnose apparently non-urinary infections?
[NS = nephrotic syndrome; SC = sieving coefficient]
3/
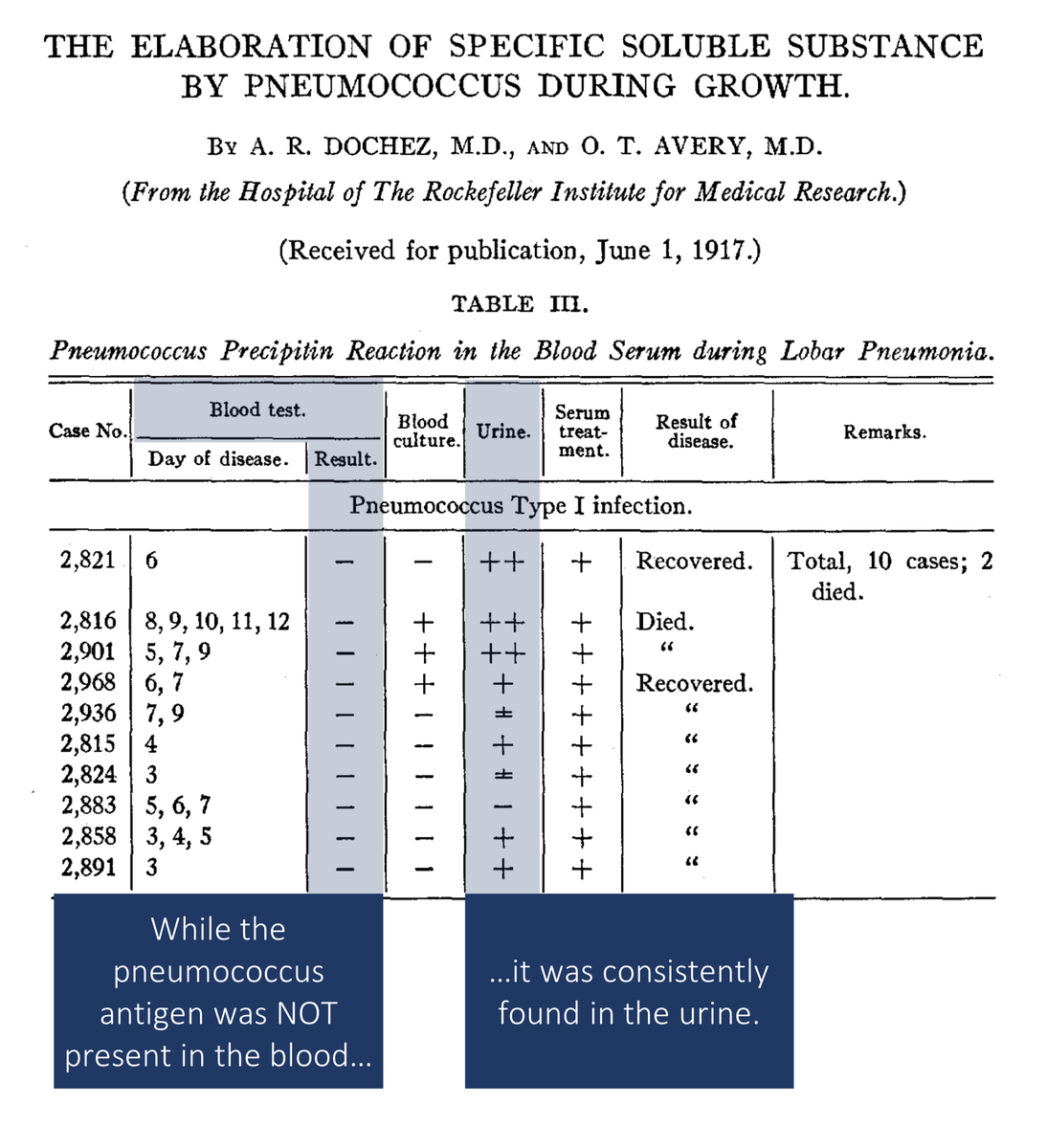
In 1917, Dochez and Avery observed that a pneumococcal antigen was readily identified in the urine of patients with lobar pneumonia, even when it couldn't be isolated in the blood.
ncbi.nlm.nih.gov/pubmed/19868163
In 1917, Dochez and Avery observed that a pneumococcal antigen was readily identified in the urine of patients with lobar pneumonia, even when it couldn't be isolated in the blood.
ncbi.nlm.nih.gov/pubmed/19868163
4/
These results from over a century ago raise two questions:
(1) How did this molecule get into the urine if pneumococcus doesn't itself infect the genitourinary system?
(2) If the molecule gets into the urine via the blood, why isn't the blood test positive too?
These results from over a century ago raise two questions:
(1) How did this molecule get into the urine if pneumococcus doesn't itself infect the genitourinary system?
(2) If the molecule gets into the urine via the blood, why isn't the blood test positive too?
5/
Before answering these questions, it's important to note that the molecule used in contemporary pneumococcal urinary antigen assays is the C-polysaccharide.
Cool fact: C-polysaccharide is what CRP "reacts" with, giving it its name, C-reactive protein.
ncbi.nlm.nih.gov/pubmed/19869788
Before answering these questions, it's important to note that the molecule used in contemporary pneumococcal urinary antigen assays is the C-polysaccharide.
Cool fact: C-polysaccharide is what CRP "reacts" with, giving it its name, C-reactive protein.
ncbi.nlm.nih.gov/pubmed/19869788
6/
In order for a molecule like to C-polysaccharide to make its way into the urine for use as a diagnostic test, two things must occur:
*filtration by the glomerular capillary
*incomplete reabsorption by the renal tubules
In order for a molecule like to C-polysaccharide to make its way into the urine for use as a diagnostic test, two things must occur:
*filtration by the glomerular capillary
*incomplete reabsorption by the renal tubules
7/
The filtration of molecules is typically quantified using the following ratio:
Concentration in the filtrate / Concentration in the plasma
This is known as the sieving coefficient (SC). The smaller the molecule, higher the SC (i.e., it is filtered more).
The filtration of molecules is typically quantified using the following ratio:
Concentration in the filtrate / Concentration in the plasma
This is known as the sieving coefficient (SC). The smaller the molecule, higher the SC (i.e., it is filtered more).

8/
Notice that sodium is completely filtered, while almost no albumin is filtered.
Based on the fact that C-polysaccharide is used as a urinary antigen for the diagnosis of pneumococcal pneumonia, which of the following are reasonable estimates for the molecular weight and SC?
Notice that sodium is completely filtered, while almost no albumin is filtered.
Based on the fact that C-polysaccharide is used as a urinary antigen for the diagnosis of pneumococcal pneumonia, which of the following are reasonable estimates for the molecular weight and SC?
9/
C-polysaccharide is ~22 kDa.
I haven't been able to find information on the radius or SC of this molecule, but we might imagine it's somewhere between myoglobin and lactoglobulin.
Conclusion: C-polysaccharide is likely filtered into the urine for us to assay.
C-polysaccharide is ~22 kDa.
I haven't been able to find information on the radius or SC of this molecule, but we might imagine it's somewhere between myoglobin and lactoglobulin.
Conclusion: C-polysaccharide is likely filtered into the urine for us to assay.

10/
C-polysaccharide is small enough to be filtered by glomerular capillaries and therefore can be picked up by urinary antigen tests.
But, why don't we just assay the blood?
One clue comes from another freely filtered polysaccharide...
...INULIN!
C-polysaccharide is small enough to be filtered by glomerular capillaries and therefore can be picked up by urinary antigen tests.
But, why don't we just assay the blood?
One clue comes from another freely filtered polysaccharide...
...INULIN!
11/
Inulin is a carbohydrate, like C-polysaccharide. If we assume that these two carbohydrates are handled similarly by the kidney, then the relative plasma and urine concentrations of inulin might provide a guide for C-polysaccharide:
Plasma = 1.0 mg/dL
Urine = 440 mg/L
Inulin is a carbohydrate, like C-polysaccharide. If we assume that these two carbohydrates are handled similarly by the kidney, then the relative plasma and urine concentrations of inulin might provide a guide for C-polysaccharide:
Plasma = 1.0 mg/dL
Urine = 440 mg/L

12/
Urine concentrations of inulin are much higher than plasma concentrations. It's possible that small microbial polysaccharide antigens have similar relative concentrations. Result:
Urine antigen test: positive
Plasma antigen test: negative
Urine concentrations of inulin are much higher than plasma concentrations. It's possible that small microbial polysaccharide antigens have similar relative concentrations. Result:
Urine antigen test: positive
Plasma antigen test: negative
13/
C-polysaccharide isn't the only small molecule antigen used for diagnosis. Others include legionella, histoplasmosis, tuberculosis, among others.
ncbi.nlm.nih.gov/pubmed/24856525
C-polysaccharide isn't the only small molecule antigen used for diagnosis. Others include legionella, histoplasmosis, tuberculosis, among others.
ncbi.nlm.nih.gov/pubmed/24856525
14/
It's worth noting that other advantages of urine exist. It is:
*easily acquired non-invasively
*large volume
*able to be concentrated
It's worth noting that other advantages of urine exist. It is:
*easily acquired non-invasively
*large volume
*able to be concentrated
15/
Before summarizing, ask the original question one more time:
Why are urine antigen tests often used to diagnose apparently non-urinary infections?
[NS = nephrotic syndrome; SC = sieving coefficient]
Before summarizing, ask the original question one more time:
Why are urine antigen tests often used to diagnose apparently non-urinary infections?
[NS = nephrotic syndrome; SC = sieving coefficient]
16/
To summarize:
⭐️many urinary antigens are small, with high sieving coefficients
⭐️this leads to their presence in the urine at high concentrations, even if the organism isn't isolated in the urine
⭐️plasma concentrations may remain low, with resulting negative assays
To summarize:
⭐️many urinary antigens are small, with high sieving coefficients
⭐️this leads to their presence in the urine at high concentrations, even if the organism isn't isolated in the urine
⭐️plasma concentrations may remain low, with resulting negative assays