,
12 tweets,
8 min read
Read on Twitter
Put on your thinking caps for this week's #PhysioQuizzo!
After finishing ID consults two weeks ago, you find yourself on renal consults. Your attending gives you two new consults:
1) 30yoM, serum Na 121, SOsm 252
2) 30yoM, serum Na 120, SOsm 253
(Questions on the next page!!!)
After finishing ID consults two weeks ago, you find yourself on renal consults. Your attending gives you two new consults:
1) 30yoM, serum Na 121, SOsm 252
2) 30yoM, serum Na 120, SOsm 253
(Questions on the next page!!!)
2/ #PhysioQuizzo
Patient #1: Na 121, SOsm 252, asymptomatic.
The attending tells you his urine Osm is 70. She asks you how you want to cure the patient's hypoNa.
You say that, before you decide, you want to know more about the patient's... [You only get 1 choice]
Patient #1: Na 121, SOsm 252, asymptomatic.
The attending tells you his urine Osm is 70. She asks you how you want to cure the patient's hypoNa.
You say that, before you decide, you want to know more about the patient's... [You only get 1 choice]
3/ #PhysioQuizzo
Patient #2: Na 120, SOsm 253, asymptomatic.
Yesterday, Patient #2 got 1L of normal saline. His SNa yesterday was 119. Urine studies today: UOsm 506, UNa 170, UK 54.
The primary team wants guidance on how much normal saline to give and how fast. You say...
Patient #2: Na 120, SOsm 253, asymptomatic.
Yesterday, Patient #2 got 1L of normal saline. His SNa yesterday was 119. Urine studies today: UOsm 506, UNa 170, UK 54.
The primary team wants guidance on how much normal saline to give and how fast. You say...
We'll post answers in 2 days when the polls end!!!
@PittIMChiefs @PittIMPD @PittIMPOCUS @OHSUIMRes @thecurbsiders @OHSUIMRes @UTSWIMchief @JMAllenbaugh @TempleIM @kidney_boy @NephroMD @IMCreighton @BostonChiefs @BrighamChiefs @BMCimRES @mgsimonson1 @MFleshner301 @akohlimd
@PittIMChiefs @PittIMPD @PittIMPOCUS @OHSUIMRes @thecurbsiders @OHSUIMRes @UTSWIMchief @JMAllenbaugh @TempleIM @kidney_boy @NephroMD @IMCreighton @BostonChiefs @BrighamChiefs @BMCimRES @mgsimonson1 @MFleshner301 @akohlimd
4/x #PhysioQuizzo
Great work everyone! Here are the solutions.
1) Patient #1: You want the HISTORY.
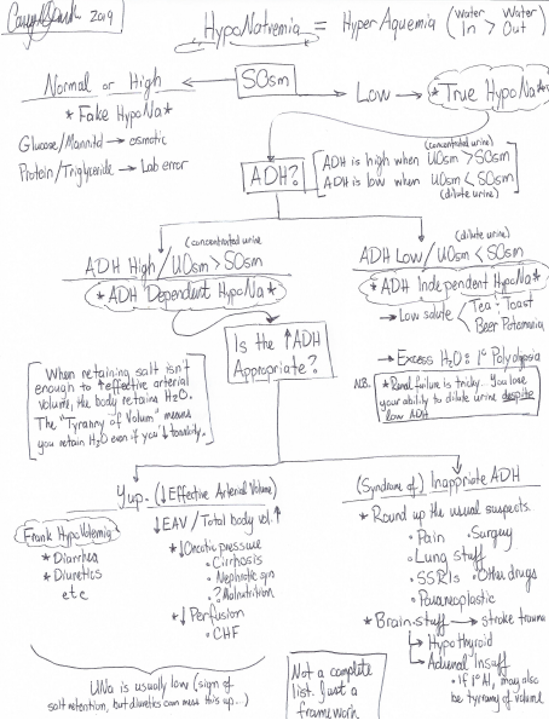
UOsm < SOsm, so this patient has an ADH *independent* cause of hyponatremia (ADH is low, urine is relatively dilute)! But what does that mean?
Great work everyone! Here are the solutions.
1) Patient #1: You want the HISTORY.
UOsm < SOsm, so this patient has an ADH *independent* cause of hyponatremia (ADH is low, urine is relatively dilute)! But what does that mean?
5/x Patient 1 solution
With dilute urine / low ADH, your Ddx is narrowed down to
- poor solute intake (beer potomania, tea and toast diet)
-excessive water intake (1* polydipsia)
A good patient history will help you decide which of these three is the culprit!
With dilute urine / low ADH, your Ddx is narrowed down to
- poor solute intake (beer potomania, tea and toast diet)
-excessive water intake (1* polydipsia)
A good patient history will help you decide which of these three is the culprit!
6/x Patient #1 solution.
A note about "Volume Status" and hyponatremia. --> It is unreliable and therefore unhelpful.
See this study: ncbi.nlm.nih.gov/pubmed/3674097
Physicians inconsistently distinguish hypovolemia from euvolemia by exam alone (correct ~47-48%). That's a coin flip!
A note about "Volume Status" and hyponatremia. --> It is unreliable and therefore unhelpful.
See this study: ncbi.nlm.nih.gov/pubmed/3674097
Physicians inconsistently distinguish hypovolemia from euvolemia by exam alone (correct ~47-48%). That's a coin flip!
7/x #PhysioQuizzo
Speaking of Volume Status and hypovolemia, nephrologist extraordinaire @NephroMD taught us a different schema for thinking about hyponatremia. We'll post our version here (what we remember) , and ask for corrections from @NephroMD and the rest of @askrenal
Speaking of Volume Status and hypovolemia, nephrologist extraordinaire @NephroMD taught us a different schema for thinking about hyponatremia. We'll post our version here (what we remember) , and ask for corrections from @NephroMD and the rest of @askrenal
8/x Sorry for misspelling polydipsia in our slide.
Anyways: Patient #2 --> You guys are right. Stop the normal saline.
Saline's osmolality is 308. The patient's UOsm = 506. They'll concentrate 1L of NS from 308 to 506, keep the remaining water and make their hypoNa worse!.
Anyways: Patient #2 --> You guys are right. Stop the normal saline.
Saline's osmolality is 308. The patient's UOsm = 506. They'll concentrate 1L of NS from 308 to 506, keep the remaining water and make their hypoNa worse!.
9/x Some brought up the idea of free water restriction for this patient. Well...
Their (UNa + UK) is > serum Na, so the FW-clearance is actually negative. (1 - [UNa+UK]/SNa) is < 0. They hold onto every drop of water they get. Instead, they need something like urea to get better
Their (UNa + UK) is > serum Na, so the FW-clearance is actually negative. (1 - [UNa+UK]/SNa) is < 0. They hold onto every drop of water they get. Instead, they need something like urea to get better
10/x What does urea or salt tabs do?
In a euvolemic patient (remember, SIADH patients are euvolemic?), they must excrete all solutes they take in. Right? So by giving them an active solute like urea or salt tabs, they must USE their own free water to dilute it and excrete it!
In a euvolemic patient (remember, SIADH patients are euvolemic?), they must excrete all solutes they take in. Right? So by giving them an active solute like urea or salt tabs, they must USE their own free water to dilute it and excrete it!
11/11 Brilliant physiology, right? We think so too. Thanks for playing this week everyone.
Let us know your comments, questions, suggestions for the future. #PhysioQuizzo
Let us know your comments, questions, suggestions for the future. #PhysioQuizzo