,
30 tweets,
9 min read
Read on Twitter
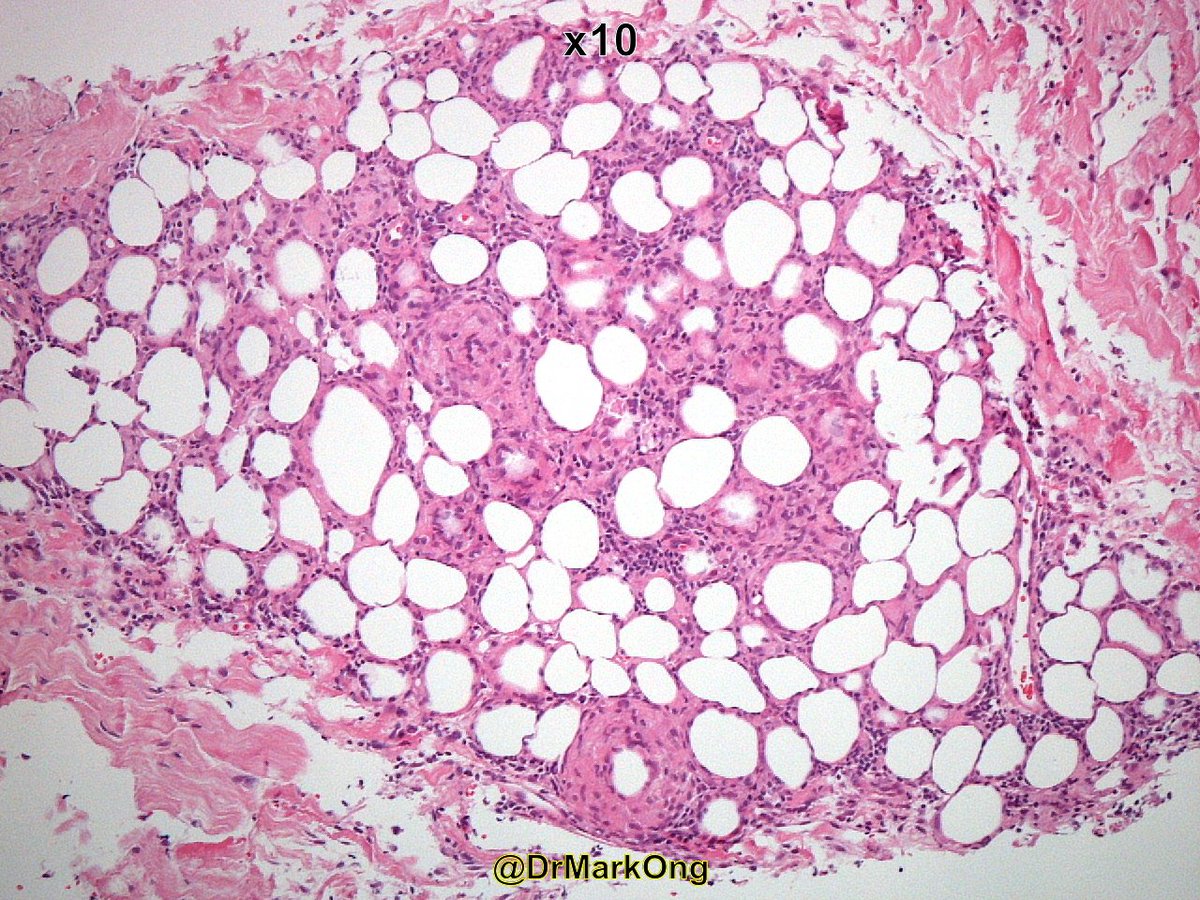
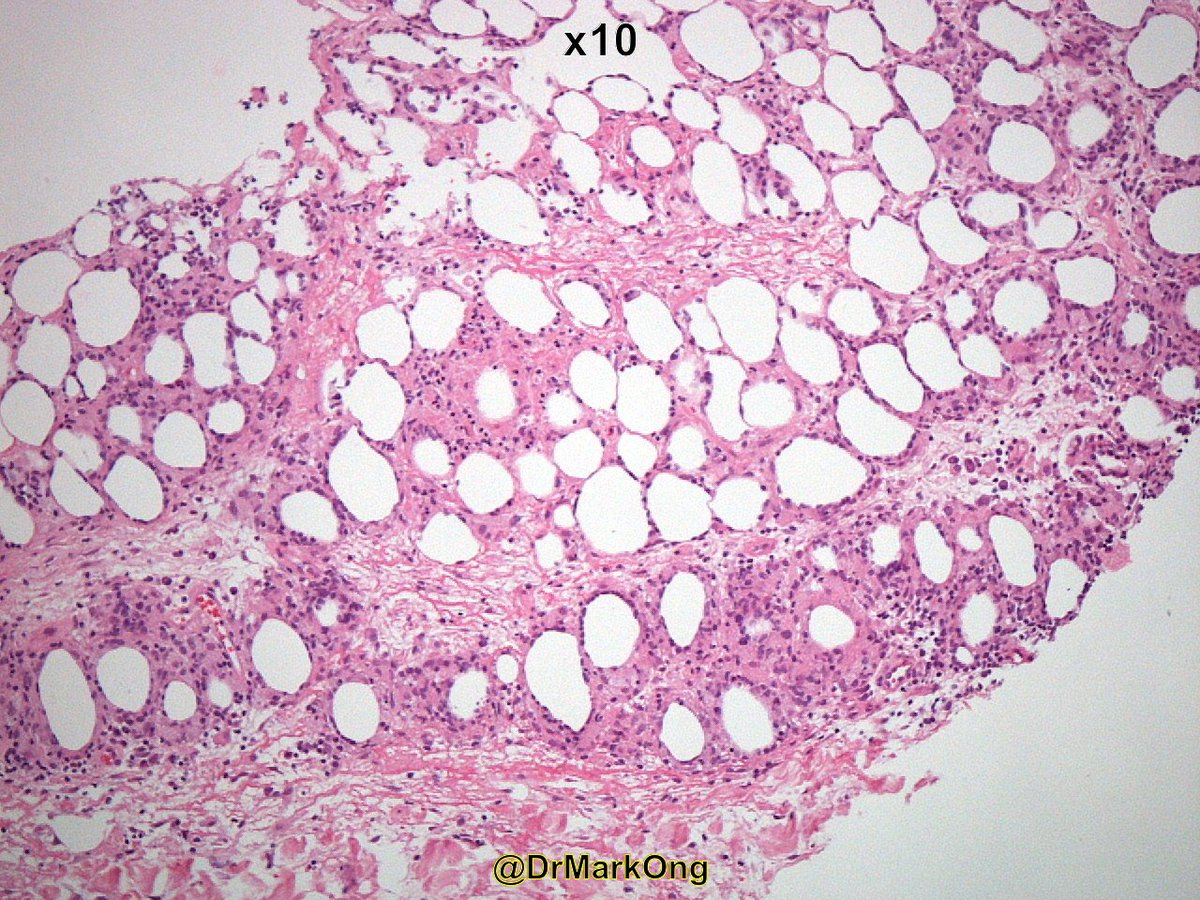
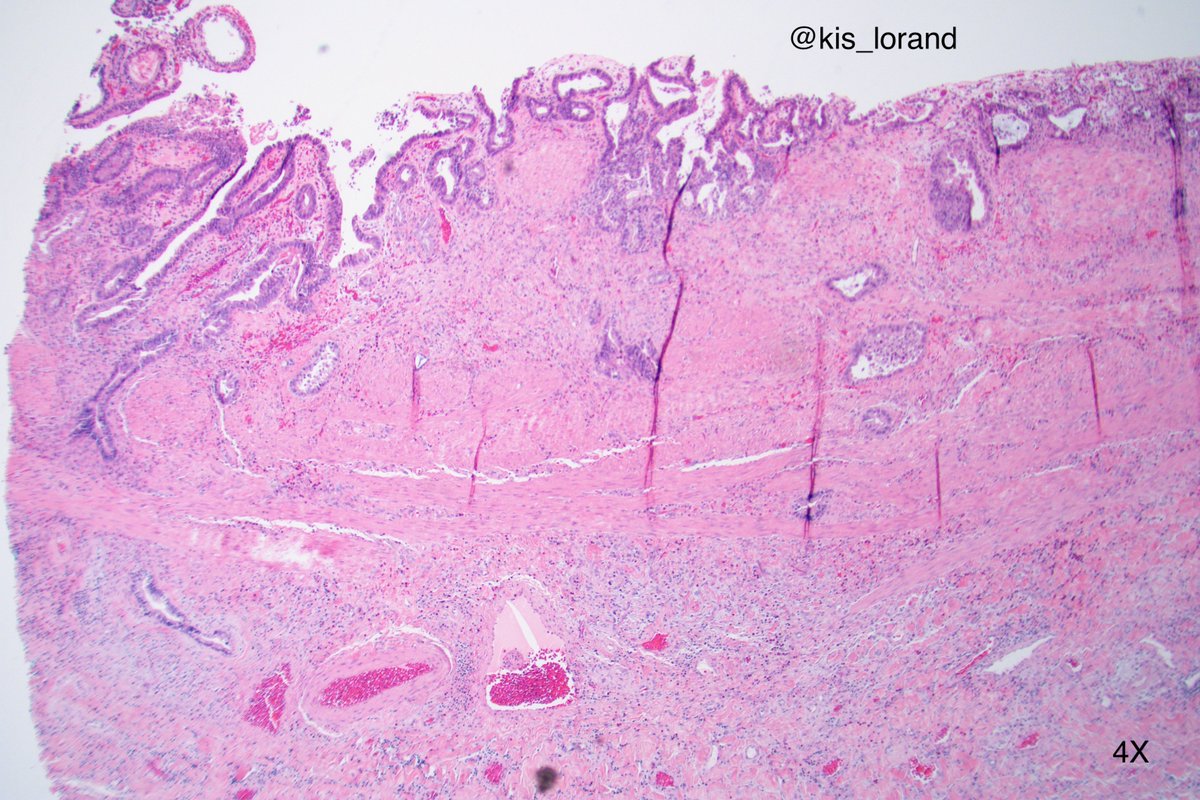
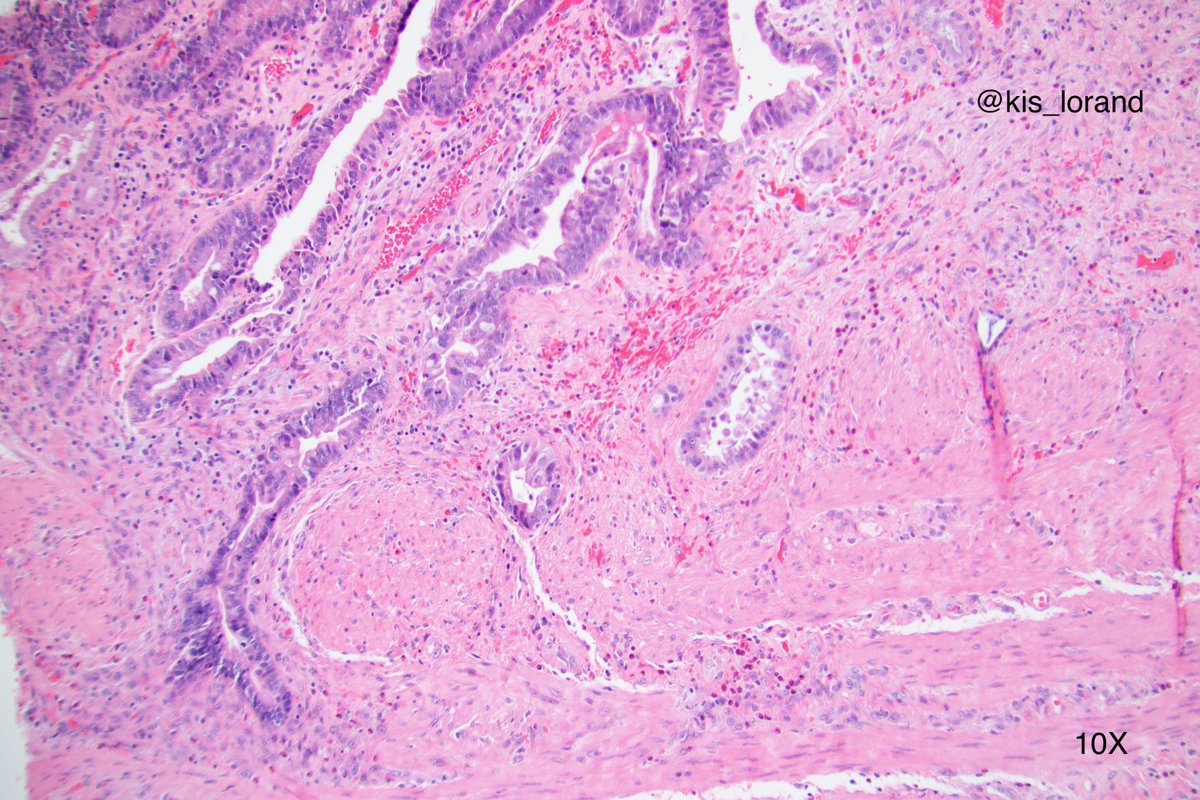
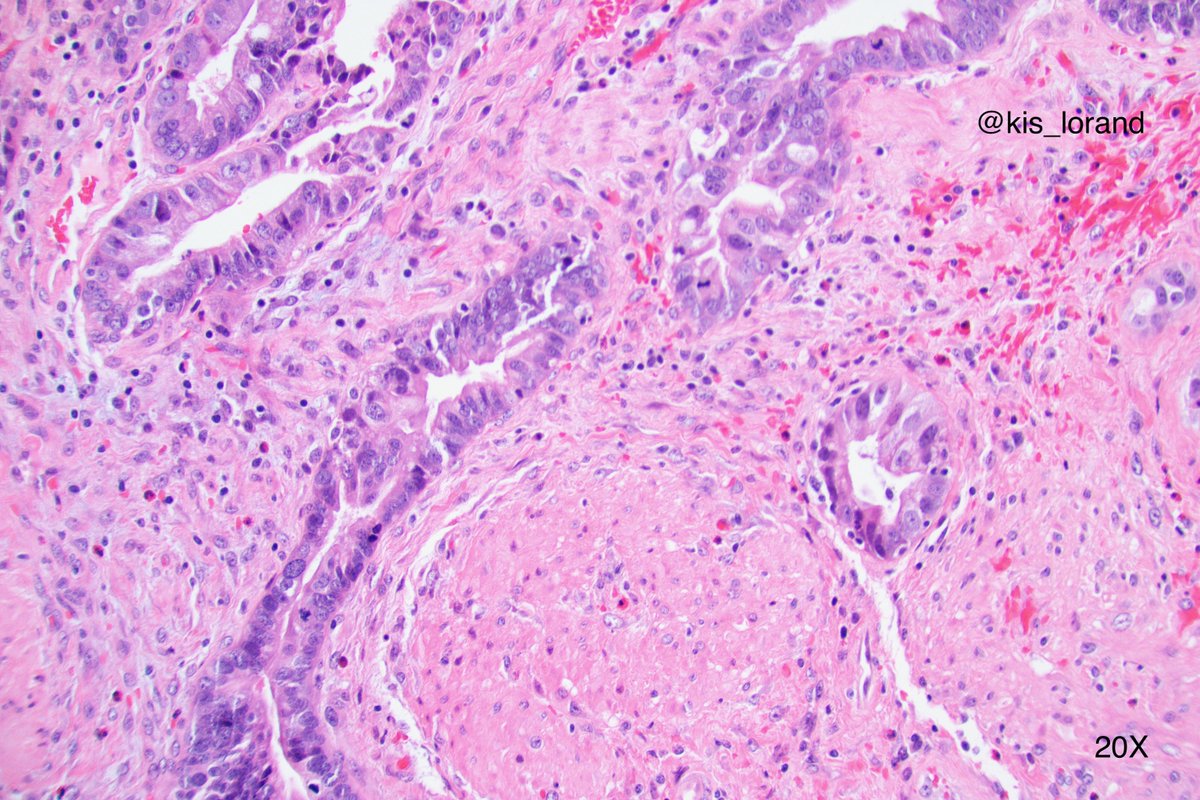
A mini case: sections from the wall of the gallbladder with the following histology...spot diagnosis 🎯
Questions in the thread...
#pathology #IHCpath
Questions in the thread...
#pathology #IHCpath
Q1: How do you interpret the p53 IHC stain? (hint: if you say "positive" then I failed as a teacher 😀😱)
Q2: In what other instances do you perform a p53 IHC?
Q2: In what other instances do you perform a p53 IHC?


It turns out that it is not a clear cut case in the provided pictures...AIS extending in Rokitansky-Aschoff sinuses has to be considered... not a gallbladder guy 😀 At the same time I would have a hard time signing out an AIS extending in RA sinuses diagnosis...
I would definitely sample more, cut levels and send the case for consultation...
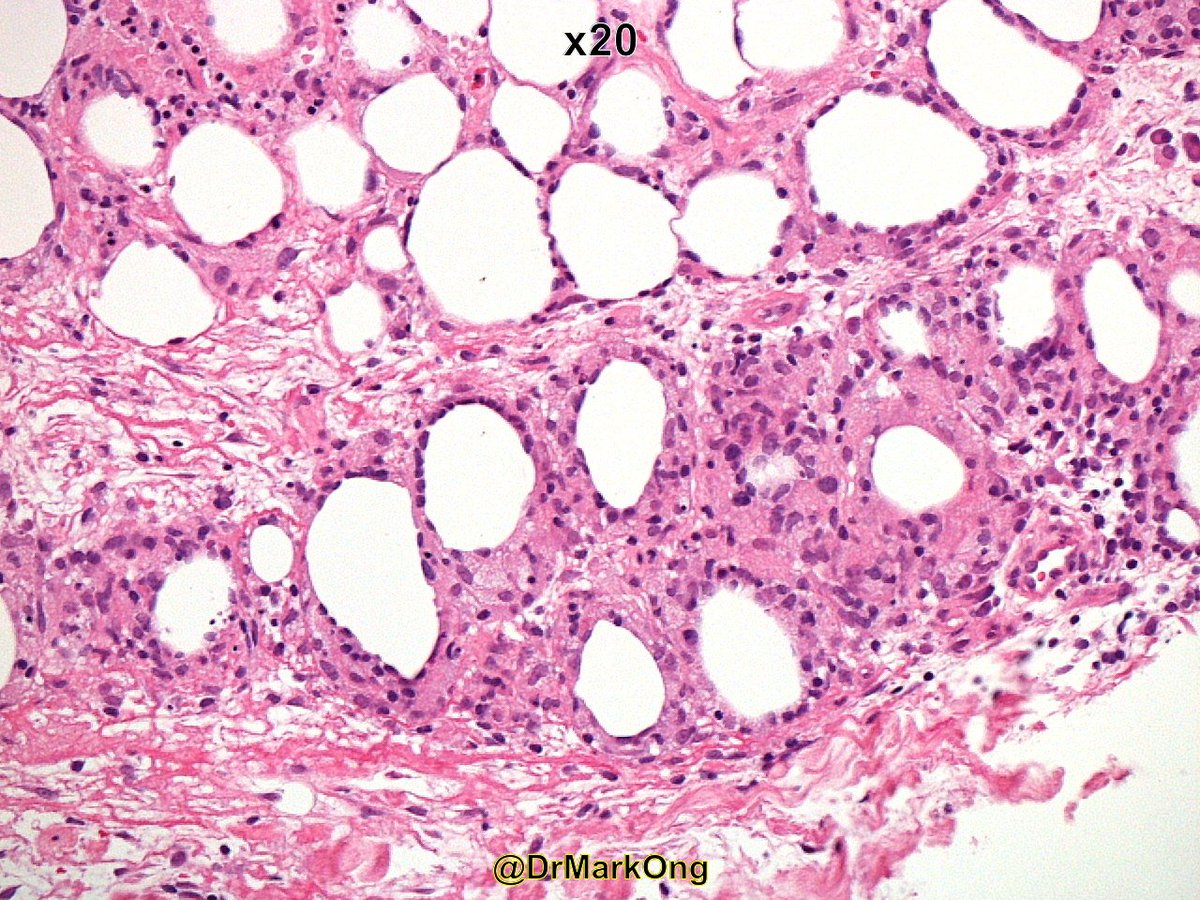
The suspicious gland is located in the subserosa where RA sinuses can also extend...Is that desmoplasia or just concentric periglandular fibrosis, not very helpful in these case...
The suspicious gland is located in the subserosa where RA sinuses can also extend...Is that desmoplasia or just concentric periglandular fibrosis, not very helpful in these case...


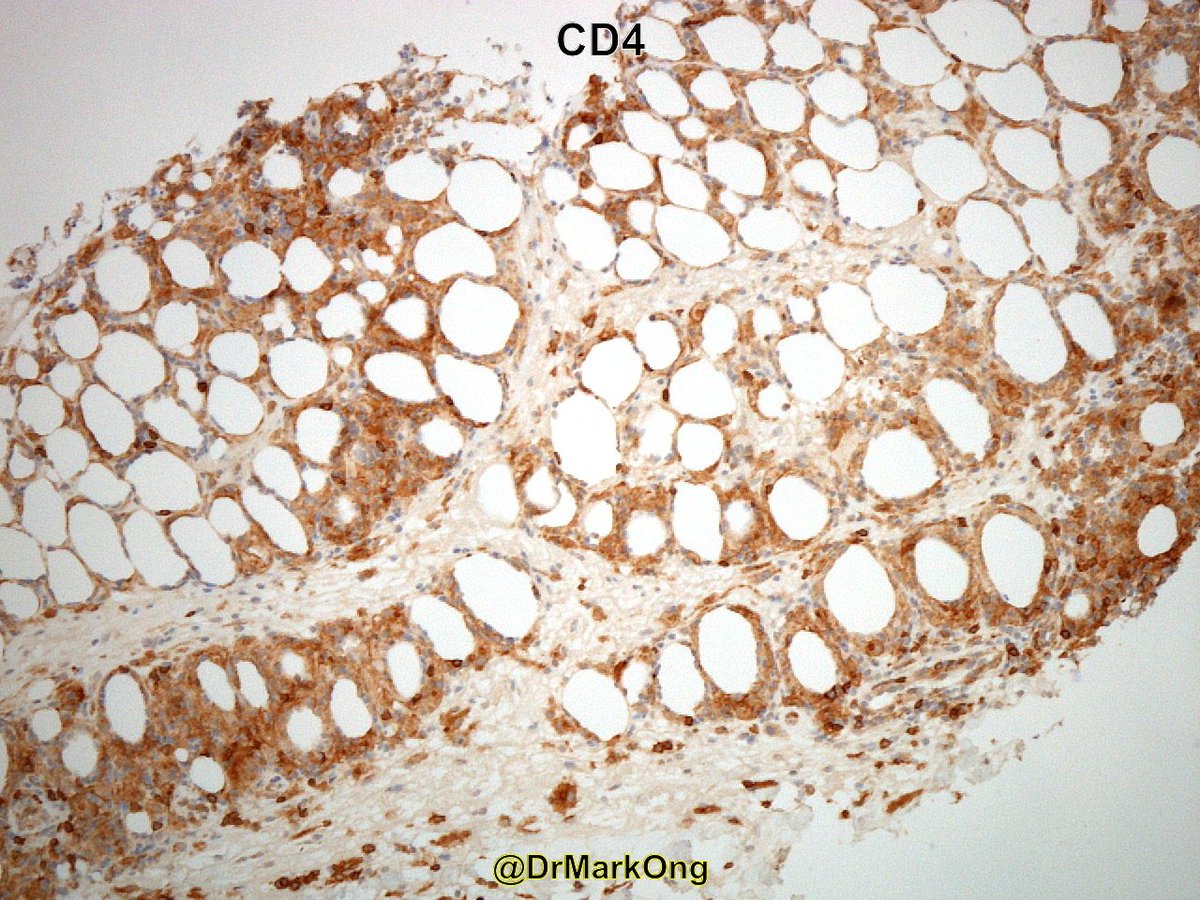
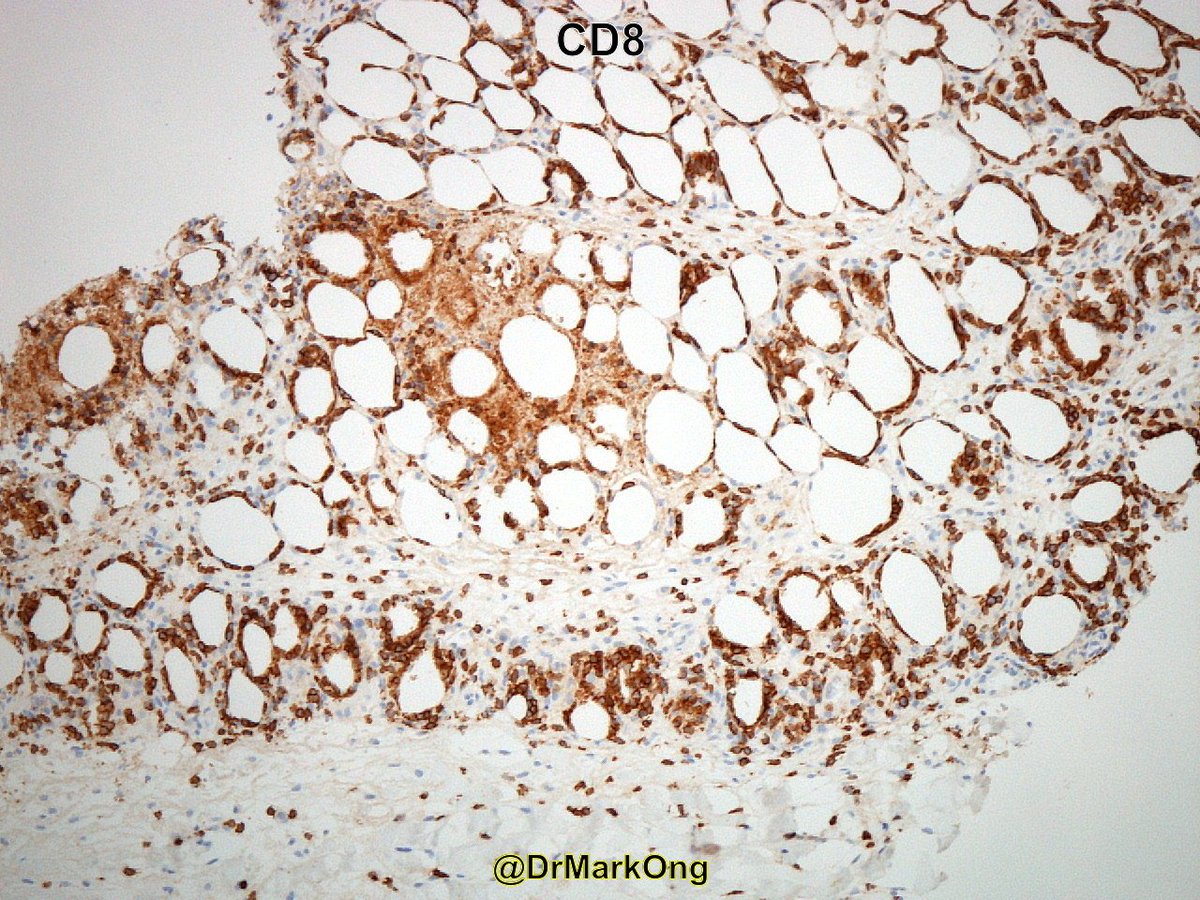
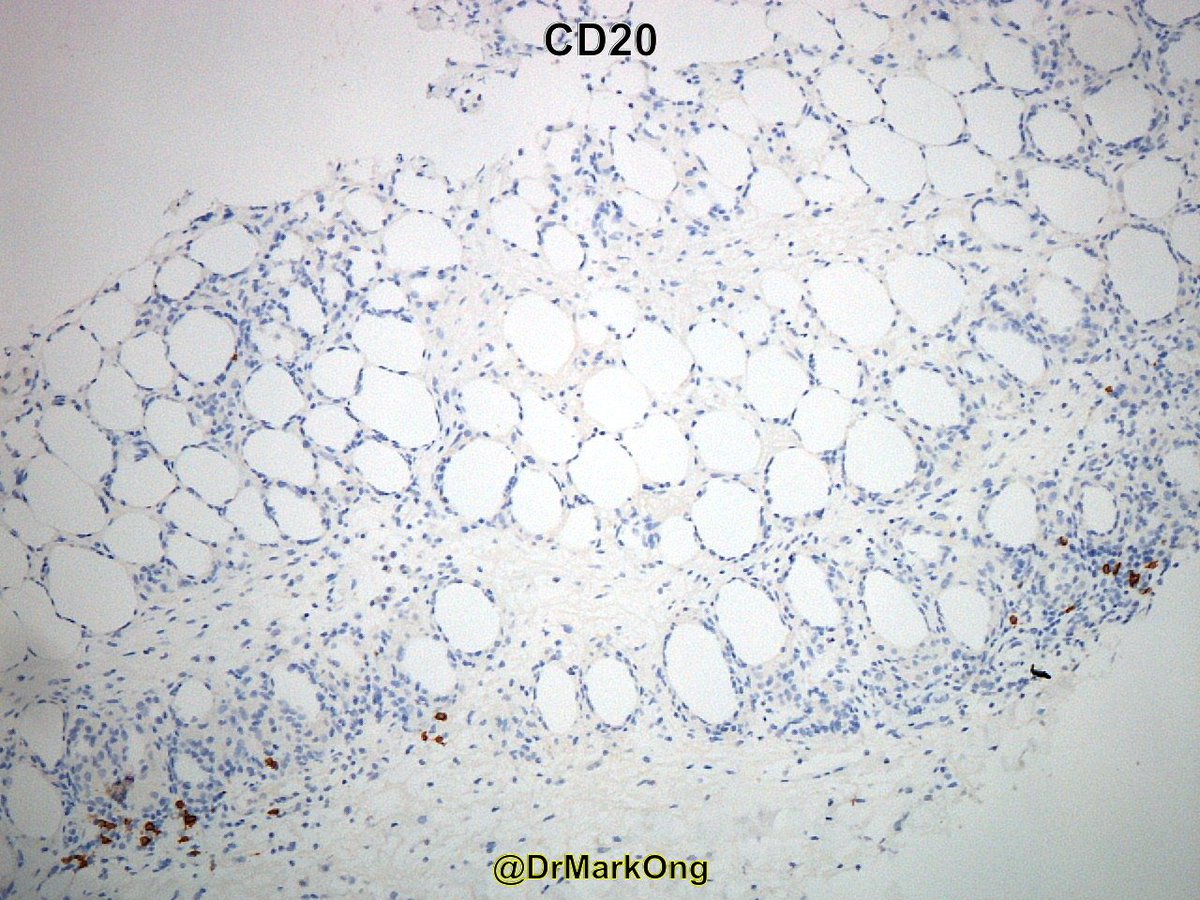
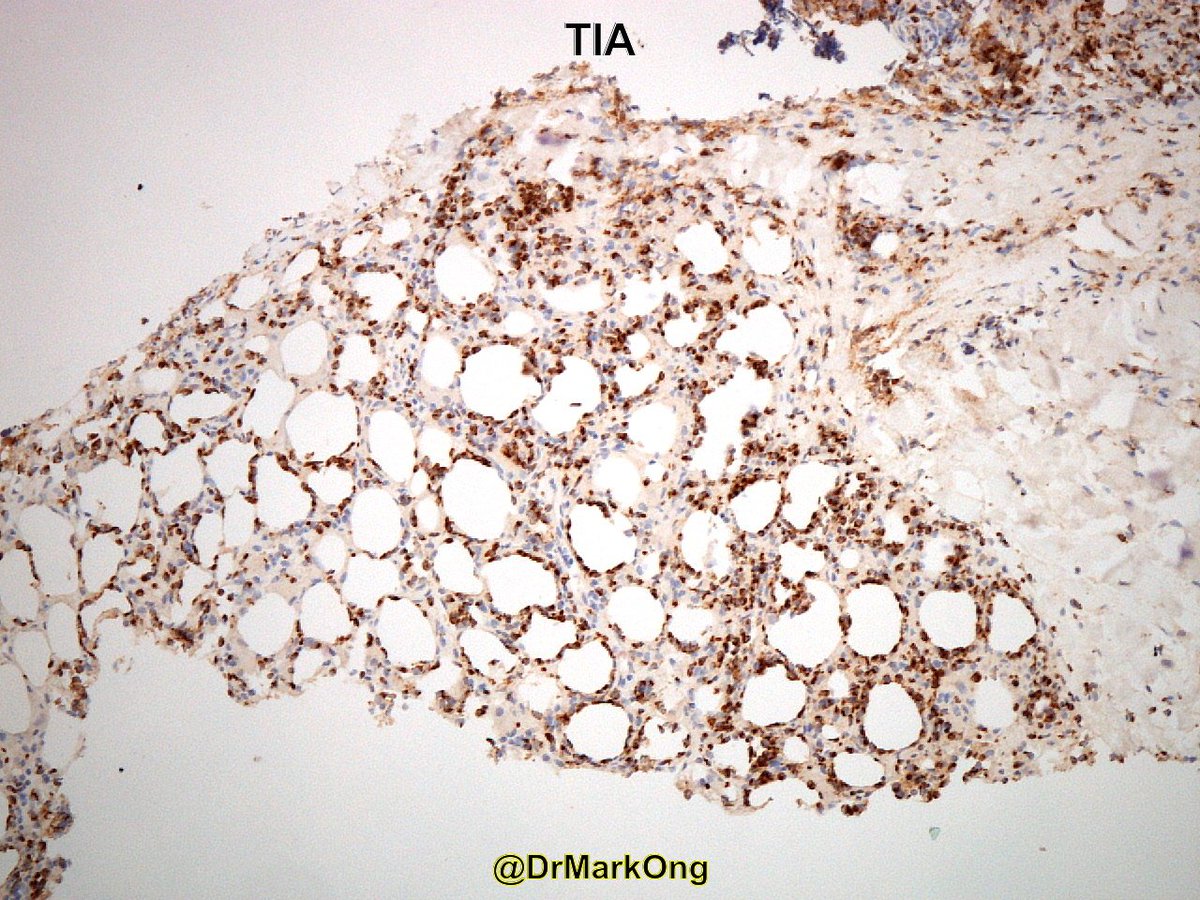
The histological features helpful in distinguishing malignant glands from benign (normal) glands are provided in the attached picture.

Some additional pictures follow from other areas of the specimen...all these glands were located subserosal... well-differentiated adenocarcinoma can be very deceptive, benign looking 😱😱



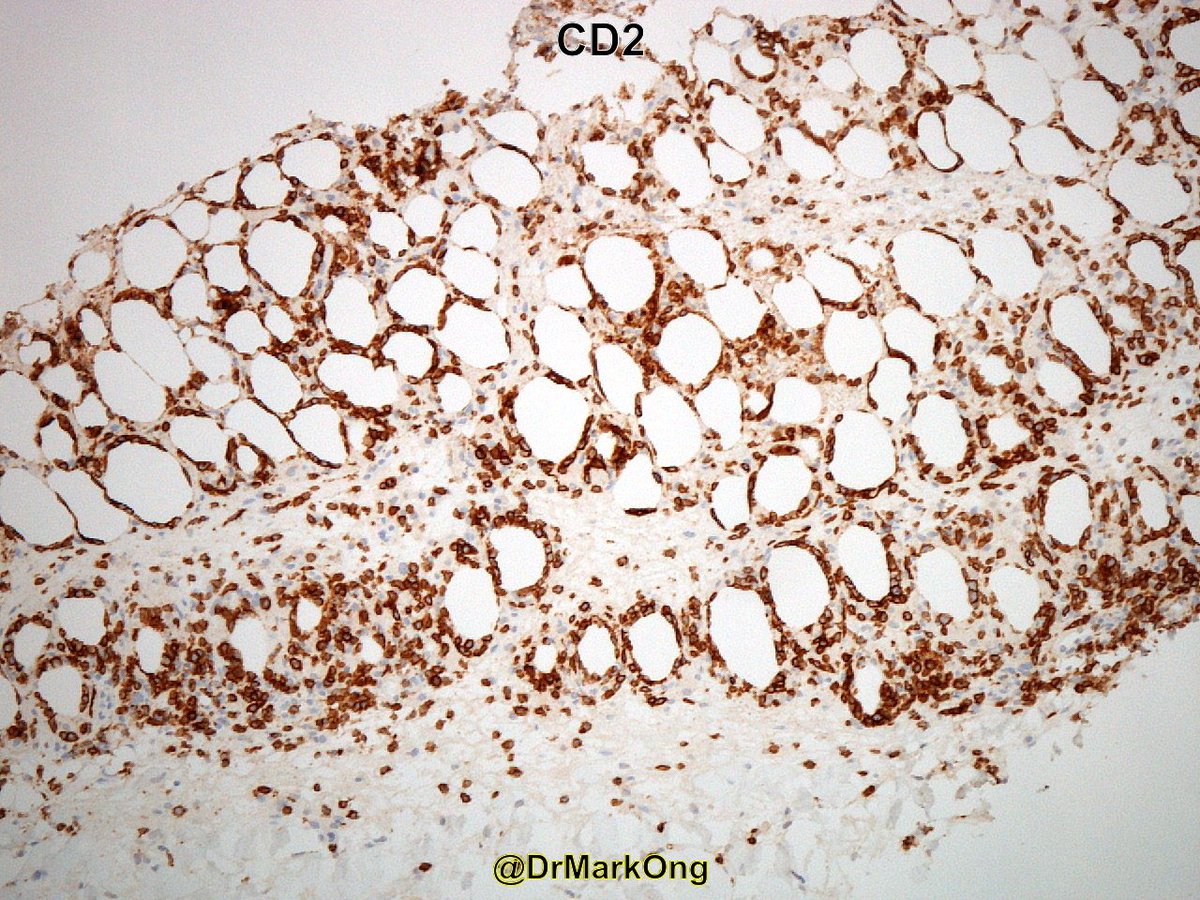
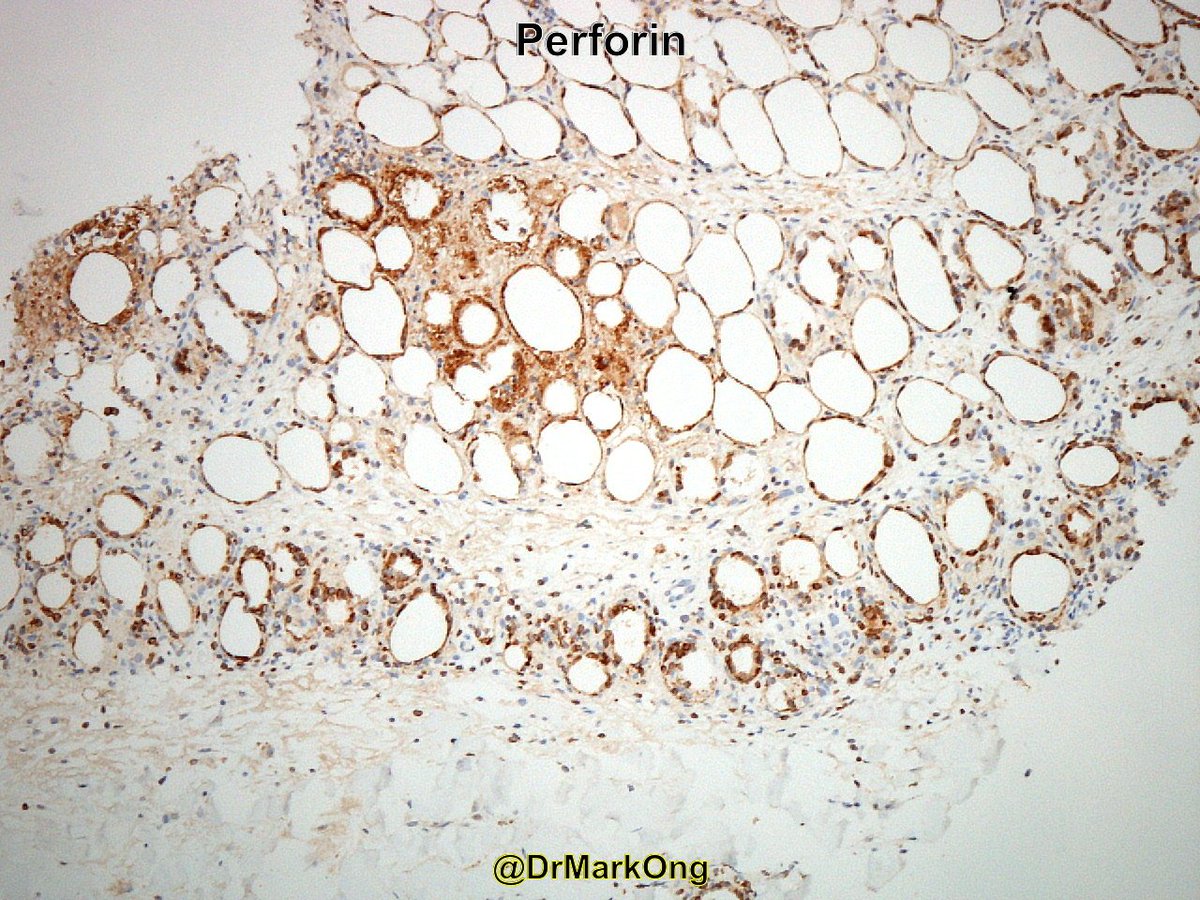
The cytokeratin IHC nicely illustrates the haphazard arrangement of the glands and the adjacent single cells.


The invasion was a side discussion, the questions were about the p53 IHC. Thanks everyone sharing your thought on how you use this IHC stain in your praxis 🙏🙏🙏 I still find it an interesting and important question!
For the interpretation part: I would describe it as "homogeneously, strongly positive consistent with mutant p53/p53 mutation" even if this expression is mostly used in the gyn pathology.
We use p53 IHC as a surrogate to p53 mutation, so basically this is the question that we indirectly want to answer with the help of this IHC.
Some of the areas where p53 IHC is used, as already mentioned by some of you, are:
Some of the areas where p53 IHC is used, as already mentioned by some of you, are:
1/ Within GU pathology some use it to distinguish reactive urothelium from CIS. I do not know of any use within prostate, testicular, or renal pathology...
A urothelial CIS case that I posted previously
A urothelial CIS case that I posted previously
2/Within GYN path:
a) distinguishing HGSC from LGSC in a small biopsy
I find p53 IHC very interesting in this ddx as it becomes a cancer subtype-specific marker favoring HGSC is mutant pattern...PAX8, WT1, ER does not differentiate these 2 cancer types...
a) distinguishing HGSC from LGSC in a small biopsy
I find p53 IHC very interesting in this ddx as it becomes a cancer subtype-specific marker favoring HGSC is mutant pattern...PAX8, WT1, ER does not differentiate these 2 cancer types...
b) distinguishing a usual cervical adenocarcinoma from a well-differentiated endometrioid endometrial adenocarcinoma (not useful for high-grade tumors in the corpus...)
I posted such a case previously...
I posted such a case previously...
c) some might use it for differentiated VIN at the surgical margins...
d) might be used to confirm the STIC diagnosis in conjunction with Ki-67
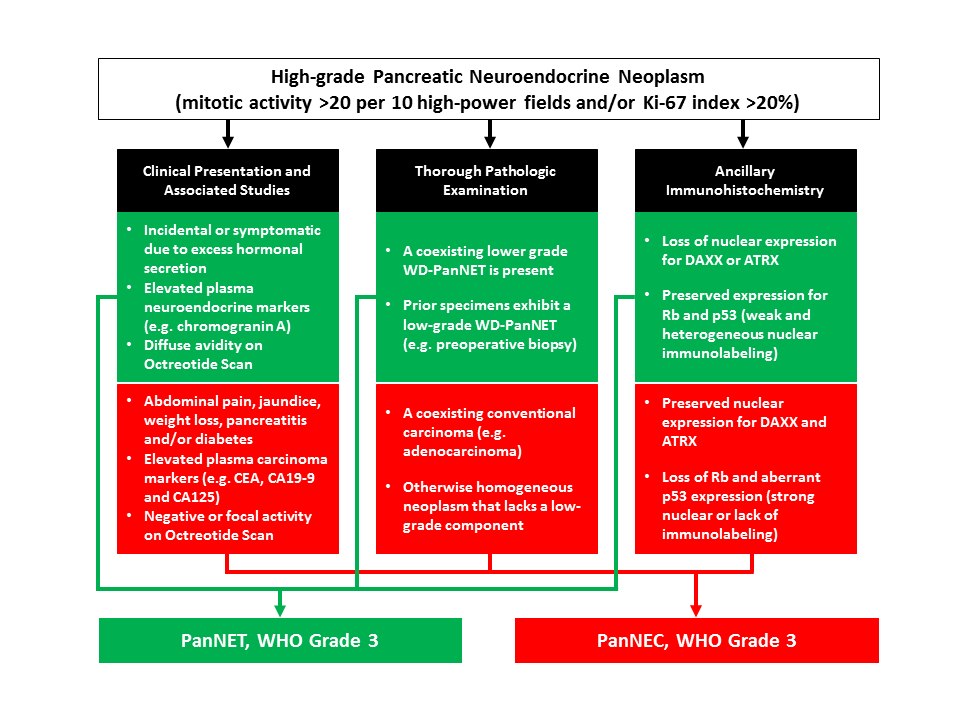
3/ In pancreas pathology:
a). used as one of the adjunct markers to differentiate between pancreatic NET WHO grade 3 from pancreatic NEC grade 3
(picture courtesy of Dr. Aatur Singhi @PancPathologist )
a). used as one of the adjunct markers to differentiate between pancreatic NET WHO grade 3 from pancreatic NEC grade 3
(picture courtesy of Dr. Aatur Singhi @PancPathologist )
b). some might use it to distinguish between chronic pancreatitis and ductal adenocarcinoma (along other markers such as SMAD4, CK17, mason, S100p, IMP3)
I mean maspin...
4/ In GI pathology used for
a) as an aid in the diagnosis of dysplasia in Barrett esophagus (BE).
In its simplest form a mutant p53 pattern would favor dysplasia (does not distinguish between LGD and HGD)
a) as an aid in the diagnosis of dysplasia in Barrett esophagus (BE).
In its simplest form a mutant p53 pattern would favor dysplasia (does not distinguish between LGD and HGD)
In the Rodger C. Haggitt GI Pathology Society recommendations on the use of ancillary stains in the diagnosis of BE published in 2017 p53 IHC was recognized as promising marker for identifying high-risk BE patients, it was not recommended for routine use at present.

Part of the problem is that there are still multiple problems with implementing p53 IHC as a routine diagnostic adjunct...

It is interesting to note that in spite of the fact that correlation of inactivating p53 mutations with the absence of p53 staining in IHC ("null mutational pattern") was know for many years the first description of this phenomenon in dysplasia was made in Barret esophagus.

Despite its shortcomings the British Society of Gastroenterology in its guidelines published in 2014 stated that "The addition of p53 immunostaining to the histopathological assessment may improve the diagnostic reproducibility of a diagnosis of dysplasia in Barrett’s oesophagus

and should be considered as an adjunct to routine clinical diagnosis (Recommendation grade C)".
Grade C recommendation requires evidence from category IV- i.e. evidence obtained from expert committee reports, or opinions or clinical experience of respected authorities- in the absence of directly applicable clinical studies.
Some basic facts on p53. 🧐
Did you know that:
➡️ germline p53 mutations lead to the Li-Fraumeni hereditary cancer predisposition syndrome
Did you know that:
➡️ germline p53 mutations lead to the Li-Fraumeni hereditary cancer predisposition syndrome
➡️ approximately 50% of Li- Fraumeni syndrome patients develop different types of cancers, including sarcoma, breast cancer, and brain cancer, by the age of 30
➡️ TP53 is commonly inactivated through missense mutations (a single nucleotide change that leads to a single amino acid change) and rarely by truncating mutations or deletions
➡️ Li-Fraumeni syndrome patients who carry a germline missense p53 mutations develop cancer at a younger age compared with patients with germline p53 deletion mutations 🙄🙄
@threadreaderapp unroll please