
Today’s #SchizoChat is all about antipsychotics. What are they, why are they useful, how are they controversial, and what do you need to know about them? #schizophrenia #schizoaffective #psychiatry
Before I begin, a quick word: this can be a very controversial topic, as we will delve in later. All folks’ opinions are valid (especially their personal experiences!) so don’t be mean! These drugs can really impact lives for the good or bad. #SchizoChat
Folks’ opinions can be very split—check out this recent poll! At the time of tweeting, the results are all over the place! Controversial! #SchizoChat
I’m not a paid representative for pharmaceutical companies—if I was, I could actually afford the pharmaceuticals I have to take. More on cost later! #SchizoChat
As usual, I’m not an expert by any means! I’m not a psychiatrist nor do I study these drugs or humans in general—I study the brains/development of non-human animals. So feel free to correct me and don’t base treatment off of my recommendations! #SchizoChat
If you have any questions at any point (even after the two-hour chat) please comment on the tweet or send me a DM—whichever makes you more comfortable! I’ll answer as soon as I can. #SchizoChat
I’m hoping to tweet at least once every 5 minutes for the next 2 hours, so check back in as I go (I’ll probably answer many of your questions later)! #SchizoChat
If you missed last week’s #SchizoChat (topic: “what is schizo?”) please check it out! I share each one as a stand-alone html and as Twitter thread—the links to both are available in my pinned thread (on my profile) or right here!
And lastly, I’ve started #SchizoChat-s to inform folks about schizo-related disorders and start a conversation. Don’t let it end with me! Please share it around to #EndTheStigma! I’ve also made some bracelets and other schizo-merch I’ll share later.
So, what are antipsychotics? What do you need to know and why should you care? Let's #SchizoChat!
As I mentioned last week, schizo-type disorders (like #schizophrenia and #schizoaffective disorder) are mental illnesses that encompass (among other things), extended periods of psychosis, where patients “lose touch with reality.” #SchizoChat
This psychosis can mean different things for different people. You may hallucinate with all five senses (hear, see, smell, feel, and/or taste things that aren’t there) and you may experience delusions about reality (i.e. god is helping me win Pokemon contests) #SchizoChat
(that's a hypothetical and definitely not something I've thought in the last few days #schizoaffective)
#SchizoChat
#SchizoChat
There are many other nasty effects of these diseases as well, including depression, cognitive decline, memory loss, loss of executive function… with #schizoaffective disorder we also get the full range of bipolar disorder symptoms
#SchizoChat
#SchizoChat
So how do you treat this? I’ll have another #SchizoChat about other treatments (next week) but in short they include medications (like antipsychotics and others), psychotherapy, special diets, and other good mental health practices like support groups and counseling
Every patient treats their illnesses their own way—you’ll need to find what fits best for you! #SchizoChat
But above all, the top recommendation for treating schizo-type disorders is medication. Dr. E. Fuller Torrey, author of “Surviving Schizophrenia” says that “drugs are the most important treatment…just as they are…for many physical illnesses.” #SchizoChat
Antipsychotics aren't just used for schizo- disorders either! Before I was diagnosed with schizoaffective disorder I was diagnosed with bipolar disorder and given an antipsychotic. Many folks know someone on antipsychotics:
#SchizoChat
#SchizoChat
I’m going to be using a lot of stats pulled from Dr. Torrey’s latest edition, as it is the most comprehensive schizo-focused book I’ve found so far (give me recommendations!) #SchizoChat #SchizoBookClub
If you recall from our last chat, we don’t really understand what “causes” schizo-type illnesses (although we have many excellent clues). In all likelihood these diagnoses are a sort of catch-all describing a set of symptoms with many different causes #SchizoChat
This means that everyone’s schizo-type disorder may function a little differently—this makes sense, as in general people are quite different. There are very few “one size fits all” treatments for any illness. #SchizoChat
As you can imagine, though, not understanding what “causes” schizo-type illnesses can make them quite tricky to treat. As Dr. Fuller points out, “drugs do not *cure*, but rather they *control* the symptoms of schizophrenia.” #SchizoChat
The really kicker (at least in my opinion) is that we don’t really understand how these drugs all work either. We have great clues, but it is really really hard to study the human brain—we can’t do many tests on humans ethically, and our mice models aren’t the same #SchizoChat
So how do you treat a disease you don’t understand well with drugs you don’t understand well? Behold, the conundrum faced with #schizophrenia and #schizoaffective disorders, along with many other diseases and mental illness! #SchizoChat
As many patients have had the misfortune to experience, this procedure is basically a trial-and-error sort of thing. Psychiatrists make their best hypotheses about which drugs they think will work the best, patients try them out and see #SchizoChat
As you can see from this #SchizoChat poll, may people frequently try five or more antipsychotics! I know that I have, and it is an awful process.
If the drugs don’t work or if the side effects are too awful you ease off those drugs and try another set. I went years and years looking for a combination that works (and mine sort of is right now? Yay me!).
#SchizoChat
#SchizoChat
The process of trying different drugs can be quite demoralizing. My lowest points in the last few years when I thought “no drugs are helping, I’m out of options, do I want to spend my life like this?” It sucks and support/therapy/counseling is super necessary
#SchizoChat
#SchizoChat
By far the most commonly used drugs are what we call “antipsychotics.” You may also hear “neuroleptics” or “major tranquilizers”—they’re all the same thing.
#SchizoChat
#SchizoChat
Do they work? You’ll hear many patients saying they don’t (or worse, they even harm you!). Unfortunately this may be the case—we don’t totally understand their impacts and, as I mentioned, folks react in different ways.
#SchizoChat
#SchizoChat
According to Dr. Torrey, 70% of patients on antipsychotics improve significantly, 20% improve minimally, and 10% don’t improve at all. More patients *not* on drugs will relapse. Not the best odds, for many patients (like me) there weren’t any other choices.
#SchizoChat
#SchizoChat
In general these drugs do best treating the “positive symptoms”—the psychosis, and do less well or even totally fail to treat the “negative symptoms”—the depression, the cognitive decline…a.k.a. the stuff that scares me the most. #SchizoChat
As Dr. Torrey emphasizes: “taking the drugs does not guarantee that the person will *not* get sick again, and *not* taking the drugs does not guarantee that a person *will* get sick, but taking the drug does…improve the odds.”
#SchizoChat
#SchizoChat
The first antipsychotic on the market was chlorpromazine. Bear with me, these drug names get complicated! Not only do you have the drug name itself (it’s generic name) but also brand names. This one goes by Thorazine or Largacitil. #SchizoChat
In general, when I talk about these drugs I’ll call them by both their generic/drug name and/or their brand name. I’ll say the generic name first in lowercase and/or the capitalized brand name. For example, chlorpromazine/Thorazine.
#SchizoChat
#SchizoChat
Chlorpromazine/Thorazine was discovered by accident, as is the case with many medicines. Researchers in France in the 1930s were looking for new anti-histamines (used to block allergy symptoms, think Claritin or Benadryl).
#SchizoChat
#SchizoChat
The drug they synthesized ended up having a sedative property (makes folks calm and sleepy). Another scientist added it to a second compound to make a drug to relax surgery patients. They mixed it a few more times and voila, an antipsychotic!
#SchizoChat
#SchizoChat
Side-note: no wonder so many folks get sleepy on antipsychotics!
I am absolutely knocked out by antihistamines-- if they're related to antipsychotics that makes sense I guess!
#SchizoChat
I am absolutely knocked out by antihistamines-- if they're related to antipsychotics that makes sense I guess!
#SchizoChat
They tested the drug on psychiatric patients (willing volunteers!) and found that it reduced mania, relaxed patients, and reduced or eliminated psychosis! So, instead of electroshock, insulin shock, or brain surgery, psychotic folks could take a pill!
#SchizoChat
#SchizoChat
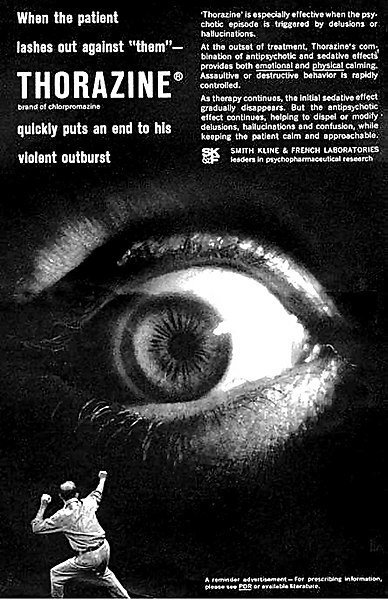
Side note, if you want nightmares check out this actual advertisement used to promote chlorpromazine/Thorazine! AAAAAAHHHH (from Wikipedia commons)
#SchizoChat
#SchizoChat
So how does this drug work? This drug and others which we call “typical antipsychotics” block dopamine receptors (D2 receptors, for you nerds out there). These receptors are the “landing point” for the brain chemical we call dopamine.
#SchizoChat
#SchizoChat
So what is dopamine, you ask? It is a chemical in your body that is technically both a hormone and a neurotransmitter—in non-technical terminology, it is a tiny molecule that acts as a signal, carrying messages from one cell to another
#SchizoChat
#SchizoChat
In the brain dopamine is released by one neuron (brain cell) and picked up (“received”) by another neuron. In this way the two cells can pass messages. The receiving neuron has special slots to pick up the dopamine—these are the “receptors.”
#SchizoChat
#SchizoChat
Drugs can block these signals from moving between cells by basically sitting on the receptor areas, keeping them from picking up the signal. It keeps the cells from talking to each other. So, “typical” antipsychotics block dopamine signals.
#SchizoChat
#SchizoChat
In popular culture we often think of dopamine as a “pleasure chemical,” the signal brains send to make you feel good about something. Why do we make drugs to block it, then?
#SchizoChat
#SchizoChat
It is perhaps more accurate to say that dopamine works to influence the motivation we have—not the motivation to do something necessarily, but the reaction we have to something.
Do we desire it? Or do we feel aversion to it? Those are dopamine messages!
#SchizoChat
Do we desire it? Or do we feel aversion to it? Those are dopamine messages!
#SchizoChat
So why does blocking dopamine reduce psychosis, prevent mood swings, etc.? That’s above my pay grade! We aren’t totally sure.
But we know that “typical” antipsychotics block dopamine reception and we know they work for some patients, somehow.
#SchizoChat
But we know that “typical” antipsychotics block dopamine reception and we know they work for some patients, somehow.
#SchizoChat
Why are we prescribing drugs that we don’t understand?
Dr. Torrey says: “The bottom line is that we really don’t know how they work. But then, we don’t yet know how aspirin works, either.”
#SchizoChat
Dr. Torrey says: “The bottom line is that we really don’t know how they work. But then, we don’t yet know how aspirin works, either.”
#SchizoChat
chlorpromazine/Thorazine also has other impacts in the brain that I’m not going to go into (comment/DM me if you want more fun brain chemical facts!) #SchizoChat
So why don’t we all just take chlorpromazine/Thorazine?
According to Wikipedia it is “an effective drug, although not a perfect one.”
There are many possible side effects—weight gain, decreased blood pressure, sedation… and many more.
#SchizoChat
According to Wikipedia it is “an effective drug, although not a perfect one.”
There are many possible side effects—weight gain, decreased blood pressure, sedation… and many more.
#SchizoChat
This makes chlorpromazine/Thorazine the rule, not the exception—these drugs have the potential to come with nasty side effects?
How nasty, you ask?
They can be life threatening or permanently disabling
#SchizoChat
How nasty, you ask?
They can be life threatening or permanently disabling
#SchizoChat
The most common permanent problems are motor control disabilities. Patients may develop unsteady Parkinson’s disease-like movements or uncontrollable eye twitches.
They are rare but they are possible.
#SchizoChat
They are rare but they are possible.
#SchizoChat
CW: suicide
Perhaps more importantly, like any mental health medication these drugs (with one possible exception) also have the possibility of increasing suicidal thoughts/ideation. It’s super dangerous and patients/caretakers need to watch for it.
#SchizoChat
Perhaps more importantly, like any mental health medication these drugs (with one possible exception) also have the possibility of increasing suicidal thoughts/ideation. It’s super dangerous and patients/caretakers need to watch for it.
#SchizoChat
Others “less dangerous” ones can still impact your quality of life. In the last three years I’ve experienced massive weight loss and gain, sedation, fainting spells, dizziness, frequent nose-bleeds, night terrors, frequent choking, lactation (ah wtf boobs?), and more
#SchizoChat
#SchizoChat
How many people experience negative side effects of antipsychotics?
Well, check out the numbers for yourself!
#SchizoChat
Well, check out the numbers for yourself!
#SchizoChat
Check out the responses to this tweet (and add your own)!
These can be NASTY!
These can be NASTY!
Why put up with such nasty side effects, you ask? Some I can’t put up with, so I try a different medication (with my psychiatrist’s help).
Others I put up with because the benefits outweigh the costs. That’s for you and your psychiatrist to decide.
#SchizoChat
Others I put up with because the benefits outweigh the costs. That’s for you and your psychiatrist to decide.
#SchizoChat
So I’ve told you a little bit about the first antipsychotic—chlorpromazine/Thorazine. There are ~17 more available, although it depends on the country in which you live.
We break them into two categories: first-gen (or “typical”) and second-gen (“atypical”).
#SchizoChat
We break them into two categories: first-gen (or “typical”) and second-gen (“atypical”).
#SchizoChat
Our buddy chlorpromazine/Thorazine falls in the first category.
These first-gen “typical” antipsychotics work, for the most part, on those dopamine receptors (although newer research continues to teach us about what these drugs actually do).
#SchizoChat
These first-gen “typical” antipsychotics work, for the most part, on those dopamine receptors (although newer research continues to teach us about what these drugs actually do).
#SchizoChat
All first-gen antipsychotics are available as generic pills at this point (they’re pre-1990) and they aren’t prescribed as frequently so even I don’t recognize all the names.
Prolizin, Haldol, Loxitane, Trilafon, Mellaril, Navane, and Stelazine. Good baby-name list. #SchizoChat
Prolizin, Haldol, Loxitane, Trilafon, Mellaril, Navane, and Stelazine. Good baby-name list. #SchizoChat
Most of these (first and second-gen) are available as shots as well. This may be preferable if you aren’t good at taking pills regularly.
As soon as I get a steady prescription I’ll likely switch because I can’t keep a good schedule.
#SchizoChat
As soon as I get a steady prescription I’ll likely switch because I can’t keep a good schedule.
#SchizoChat
The second-gen categories came out after 1990—they’re also called “atypical” because we thought they worked differently (targeted something other than dopamine receptors) but more recent understanding has sort of blown holes in that ship.
#SchizoChat
#SchizoChat
These second-gen drugs still target dopamine receptors but also others (like serotonin receptors, GABA receptors—other brain communication paths, basically) and may have a lower risk of those aforementioned motor control disabilities
#SchizoChat
#SchizoChat
Again, though, we still don’t know a lot about these drugs.
Second-gen antipsychotics likely aren’t better than first-gen and they probably work on similar pathways.
Patients need to find the one that fits them best from either category.
#SchizoChat
Second-gen antipsychotics likely aren’t better than first-gen and they probably work on similar pathways.
Patients need to find the one that fits them best from either category.
#SchizoChat
These second-gen drugs are likely more familiar—brand names like Abilify, Saphris, Fanapt, Latuda, Zyprexa, Invega, Seroquel, Risperdal, Geodon. Many don’t have generics.
They’re also great baby names.
#SchizoChat
They’re also great baby names.
#SchizoChat
Some of these drugs boast other benefits too—Latuda, the drug I’m currently taking, can also have stabilizing effects (reducing mania and depression). So maybe it’ll help my bipolar symptoms too.
Maybe.
#SchizoChat
Maybe.
#SchizoChat
Psychiatrists can also combine these antipsychotics with other drugs—other antidepressants, anti-anxiety meds, mood stabilizers, etc.
I take a total of five different medications a day. I’ll talk about that more next week!
#SchizoChat
I take a total of five different medications a day. I’ll talk about that more next week!
#SchizoChat
Another intriguing second-gen antipsychotic is called clozapine/Clozaril—the first second-gen drug. It’s often given as a “last resort” option for folks who aren’t benefited by other antipsychotics. But intriguingly, it can often be the most helpful!
How?
#SchizoChat
How?
#SchizoChat
CW: suicide
Well, clozapine/Clozaril is the only antipsychotic we know of that reduces the rate of suicidal behavior.
So why isn’t everyone on this drug?
#SchizoChat
Well, clozapine/Clozaril is the only antipsychotic we know of that reduces the rate of suicidal behavior.
So why isn’t everyone on this drug?
#SchizoChat
Clozapine/Clozaril can cause a sudden decrease in low white blood cell counts, which suppresses immunity and can lead to death.
Approximately 1% of the patients on this drug develop these symptoms.
#SchizoChat
Approximately 1% of the patients on this drug develop these symptoms.
#SchizoChat
Because of this, the vast majority of prescribers do not even mention clozapine/Clozaril.
If you are prescribed this drug (at least in the U.S.) you are required to do weekly blood tests initially then monthly blood tests afterward.
#SchizoChat
If you are prescribed this drug (at least in the U.S.) you are required to do weekly blood tests initially then monthly blood tests afterward.
#SchizoChat
Because of this complication, clozapine is rarely mentioned. At least at the time of tweeting, the majority of folks responding to this poll have never heard of it-- and this is #MentalHealth Twitter!
#SchizoChat
#SchizoChat
It’s intriguing (at least to me) that one of the most (potentially) helpful antipsychotics is so rarely prescribed.
Here is more info in case you are interested:
vice.com/en_us/article/…
#SchizoChat
Here is more info in case you are interested:
vice.com/en_us/article/…
#SchizoChat
So across the board, many antipsychotics.
They work in different ways, they cost different amounts… bottom line, patients/caretakers need to find one that is right for them, and it often takes a depressingly long period of trial-and-error.
#SchizoChat
They work in different ways, they cost different amounts… bottom line, patients/caretakers need to find one that is right for them, and it often takes a depressingly long period of trial-and-error.
#SchizoChat
Plus, as you grow and change, as the seasons change, etc., your pills may not be as well-matched to your biology as they were in the past.
So patients need to keep checking in to make sure that their drugs are working! So much work.
#SchizoChat
So patients need to keep checking in to make sure that their drugs are working! So much work.
#SchizoChat
And little is known of the effect of most of these drugs on developing fetuses, so patients on antipsychotics need to work with their psychiatrist to determine what is the best option during pregnancy/breastfeeding #SchizoChat
Why are antipsychotics controversial? There are many reasons (I’ll go in more detail below), but especially 1. Negative side-effects, 2. Effectiveness, 3. Consent, 4. General aversion to medication, and 5. Cost.
#SchizoChat
#SchizoChat
I’ve already mentioned the first couple of controversies: these drugs can come with some nasty side effects. Some people experience long-lasting side effects or even permanent ones.
I can’t blame people for being hurt, scared, angry, and everything in-between!
#SchizoChat
I can’t blame people for being hurt, scared, angry, and everything in-between!
#SchizoChat
I’ve also mentioned that they vary in effectiveness. Just as different patients likely have different root “causes” of schizo-type disorders, different patients respond to drugs in different ways.
One drug may be perfect for one patient, awful for another
#SchizoChat
One drug may be perfect for one patient, awful for another
#SchizoChat
And we know that for a minority of patients (~10%) none of the drugs we currently have will be effective at all.
Running the gauntlet of constantly trying new drugs is exhausting and you may never find an answer.
It sucks.
#SchizoChat
Running the gauntlet of constantly trying new drugs is exhausting and you may never find an answer.
It sucks.
#SchizoChat
So ultimately it becomes a cost-benefit analysis.
How much is this drug hurting vs. helping?
Again, ideally, this would be up to the patients and their psychiatrists, but that brings me to my next point: consent.
#SchizoChat
How much is this drug hurting vs. helping?
Again, ideally, this would be up to the patients and their psychiatrists, but that brings me to my next point: consent.
#SchizoChat
Approximately half of schizo-type patients are aware of their illness and can work with psychiatrists and their families to find medications, adjust their doses, and report their side effects.
I luckily fall into this category (for now)
#SchizoChat
I luckily fall into this category (for now)
#SchizoChat
Even then, though, it isn’t easy!
Many of us deal with memory loss, heavy sedation, problems with sleep schedules—it makes it very hard to remember to take the drugs on time and correctly (with food, without food, at the right time, etc.)
#SchizoChat
Many of us deal with memory loss, heavy sedation, problems with sleep schedules—it makes it very hard to remember to take the drugs on time and correctly (with food, without food, at the right time, etc.)
#SchizoChat
Unfortunately, the other half of schizo-type patients have varying degrees of what we call “anosognosia”—in simple terms, the patient is unaware of their mental illness or the seriousness of it.
#SchizoChat
#SchizoChat
This unawareness is most often associated with bipolar disorder or schizo-type disorders (although remember it is not all of us!).
While it is often viewed as “stubbornness” or “denial,” it is not—it is literally the result of illness-based brain changes.
#SchizoChat
While it is often viewed as “stubbornness” or “denial,” it is not—it is literally the result of illness-based brain changes.
#SchizoChat
This unawareness may be temporary—patients may not recognize that they are in a psychotic break or in a manic state.
Other times it can be much more long-term—it depends on the patient.
#SchizoChat
Other times it can be much more long-term—it depends on the patient.
#SchizoChat
As you can imagine, it can be really really problematic to treat someone who doesn’t recognize that they are experiencing symptoms of a major mental illness.
Not only do you have to decide that they are ill (definitely not error-proof) but you have to treat it.
#SchizoChat
Not only do you have to decide that they are ill (definitely not error-proof) but you have to treat it.
#SchizoChat
In these cases, family members or concerned parties will act on the ill person’s behalf to make decisions (or in many cases, ER doctors and institutional staff).
The careful balance of weighing costs and benefits is no longer up to the patient
#SchizoChat
The careful balance of weighing costs and benefits is no longer up to the patient
#SchizoChat
This lack of patient consent and control is obviously very problematic and I’ll dedicate a whole upcoming #SchizoChat to the topic, but just I cannot imagine how traumatizing that must be, especially with the potential for nasty lasting side-effects!
Side point: this is one of the many reasons why the idea of being hospitalized/institutionalized can be terrifying and traumatic.
The week after next my theme will be “Asylums and Halloween,” talking about the realities and representations of institutionalization
#SchizoChat
The week after next my theme will be “Asylums and Halloween,” talking about the realities and representations of institutionalization
#SchizoChat
Long-story-short: if you are planning on being a “lunatic,” a “psycho,” or a straight-jacket-bound person for Halloween, think critically about your costume, its history, its ableism, and its effect on actual psychotic folks.
#SchizoChat
#SchizoChat
In addition to this cost-benefit analysis and major consent problems, some folks just don’t like taking medication.
My mom is one of those people that just doesn’t like ingesting drugs.
How do we treat them?
#SchizoChat
My mom is one of those people that just doesn’t like ingesting drugs.
How do we treat them?
#SchizoChat
In addition, remember that a common symptom of psychosis is delusions.
Patients may believe that they are being poisoned by spies or followed through datachips in their pills.
They may resist taking them.
#SchizoChat
Patients may believe that they are being poisoned by spies or followed through datachips in their pills.
They may resist taking them.
#SchizoChat
This comes back to that cost-benefit analysis.
Does the emotional/psychological cost of taking the medication outweigh the benefit?
If so, it definitely warrants a serious conversation about the use of antipsychotics.
#SchizoChat
Does the emotional/psychological cost of taking the medication outweigh the benefit?
If so, it definitely warrants a serious conversation about the use of antipsychotics.
#SchizoChat
If you can't see the rest of the thread after this check it out here-- not sure how I messed it up!
second part:
second part:
And finally: the costs. The actual dollar-sign costs of antipsychotic medication. For clarity, I’m in the United States, where the cost of medication comes out of pocket or in the form of a scaled “co-pay” with the insurance paying a portion and the patient the rest.
#SchizoChat
#SchizoChat
Antipsychotics are a HUGE business for pharmaceutical companies.
In 2010 sales of those 18 antipsychotic drugs totaled $16 BILLION. With a “b.”
They are often Big Pharma companies’ best-selling drugs.
#SchizoChat
In 2010 sales of those 18 antipsychotic drugs totaled $16 BILLION. With a “b.”
They are often Big Pharma companies’ best-selling drugs.
#SchizoChat
In other words, “treating schizophrenia is a big business,” with all of the problems that any big capitalist business brings.
These are a product.
A product that patients desperately need, but also a product lining company pockets.
#SchizoChat
These are a product.
A product that patients desperately need, but also a product lining company pockets.
#SchizoChat
Because the United States does not cap the profit that pharmaceutical companies can make off of drug sales, these drugs are often 2-4x more expensive in the U.S. than in other countries (I mostly know about Europe but would love other perspectives) #SchizoChat
When a product comes out it comes out as a brand name—that one brand controls the market until their patent expires.
Patents usually last for 20 years, an exhaustingly long time to wait for a cheaper generic.
#SchizoChat
Patents usually last for 20 years, an exhaustingly long time to wait for a cheaper generic.
#SchizoChat
Plus, assuming you have U.S. insurance, there is no guarantee they will agree to cover your drug, generic or brand-name.
My psychiatrist submitted my last prescription with the words: “fingers crossed! If not approved it’ll be $6000/month." You know, reasonable!
#SchizoChat
My psychiatrist submitted my last prescription with the words: “fingers crossed! If not approved it’ll be $6000/month." You know, reasonable!
#SchizoChat
Newer drugs are more expensive and less likely to be approved, so my psychiatrists tried me on the cheaper, less expensive ones first.
I couldn’t get them to work. #SchizoChat
I couldn’t get them to work. #SchizoChat
My insurance did approve the medication for a whopping $300 copay a month (with good insurance!), although luckily the brand (Latuda) offers a coupon on their website that brought it down to $15 monthly (the one time I’ve been happy with them).
#SchizoChat
#SchizoChat
I’ve heard this same story over and over. They are SO EXPENSIVE.
Plus, schizo- symptoms often make it hard to hold down a regular job. Without a consistent paycheck and employer insurance, antipsychotics are often just out-of-reach.
#SchizoChat
Plus, schizo- symptoms often make it hard to hold down a regular job. Without a consistent paycheck and employer insurance, antipsychotics are often just out-of-reach.
#SchizoChat
How do we fix this?
A lot of the problem is legislative—drug companies need to be help accountable and need to make drugs more accessible.
We also need to raise awareness—if folks think this is important they’ll fund research to find better drugs!
#SchizoChat
A lot of the problem is legislative—drug companies need to be help accountable and need to make drugs more accessible.
We also need to raise awareness—if folks think this is important they’ll fund research to find better drugs!
#SchizoChat
So, in conclusion—antipsychotics.
They may be working super well for you and that is great!
It’s only been three weeks but my Latuda has basically rendered me psychosis-free and has significantly raised my mood…so far.
#SchizoChat
They may be working super well for you and that is great!
It’s only been three weeks but my Latuda has basically rendered me psychosis-free and has significantly raised my mood…so far.
#SchizoChat
They may also work really poorly.
They may not help at all or they may have awful side effects.
In general, everyone’s experience is different and we can’t discount each other’s experiences, good or bad.
#SchizoChat
They may not help at all or they may have awful side effects.
In general, everyone’s experience is different and we can’t discount each other’s experiences, good or bad.
#SchizoChat
They’re expensive, their application can be problematic, finding the right one is like pulling teeth (for years), but in many cases they are the best way to fight the symptoms of psychosis.
#SchizoChat
#SchizoChat
Want to learn more?
As usual, I recommend Dr. Torrey’s Surviving Schizophrenia, where I pulled a lot of these stats (to be honest the rest were generally just Google searches).
Ask me more questions please!! And give me your perspective!!
#SchizoChat
As usual, I recommend Dr. Torrey’s Surviving Schizophrenia, where I pulled a lot of these stats (to be honest the rest were generally just Google searches).
Ask me more questions please!! And give me your perspective!!
#SchizoChat
If you want to help us grow #SchizoChat and other schizo-awareness efforts, stay tuned!
I’m slowly building a website, a letter-writing campaign, and (hopefully) an Etsy store.
In the meantime, I have bracelets! DM me a shipping address.
I’m slowly building a website, a letter-writing campaign, and (hopefully) an Etsy store.
In the meantime, I have bracelets! DM me a shipping address.
And as usual, please share these posts and my other schizo-related shitposts around.
The more people thinking about schizo the closer we are to educating them and ending the stigma!
#SchizoChat
The more people thinking about schizo the closer we are to educating them and ending the stigma!
#SchizoChat
Also, please respond to this poll!
I forgot to mention, the bracelets are first-come-first-serve. I have, like, five. If enough folks are interested I can buy more but I don't have the cash so they'd be like $5 each.
I forgot to mention, the bracelets are first-come-first-serve. I have, like, five. If enough folks are interested I can buy more but I don't have the cash so they'd be like $5 each.
That concludes our #SchizoChat!
Next week’s topic will be “other treatments,” and the week after will be “Asylums and Halloween,” as it is the day before my favorite holiday.
Tweet you then!
Next week’s topic will be “other treatments,” and the week after will be “Asylums and Halloween,” as it is the day before my favorite holiday.
Tweet you then!
hey @threadreaderapp can I get this unrolled please? I want to share it with folks!














