
This is quiz day for my medics. Spot diagnosis only. Dermatology residents and consultants are exempted from this.
Let's go.
1. 5 year history of lesions on the face. Asymptomatic
What is your diagnosis?
Let's go.
1. 5 year history of lesions on the face. Asymptomatic
What is your diagnosis?

2. Recurrent history of itching on the exposed areas of the limbs. In a 6 year old that started 2 years ago. Commonly starts as papules that ulcerate after itching to leave behind dark spots. Diagnosis?

3. Itchy lesions particularly worse at night. Lives in Apple island with the parents but went for camp 4 weeks prior. Similar lesions in her nanny and father. Also noted in the groin. Diagnosis?

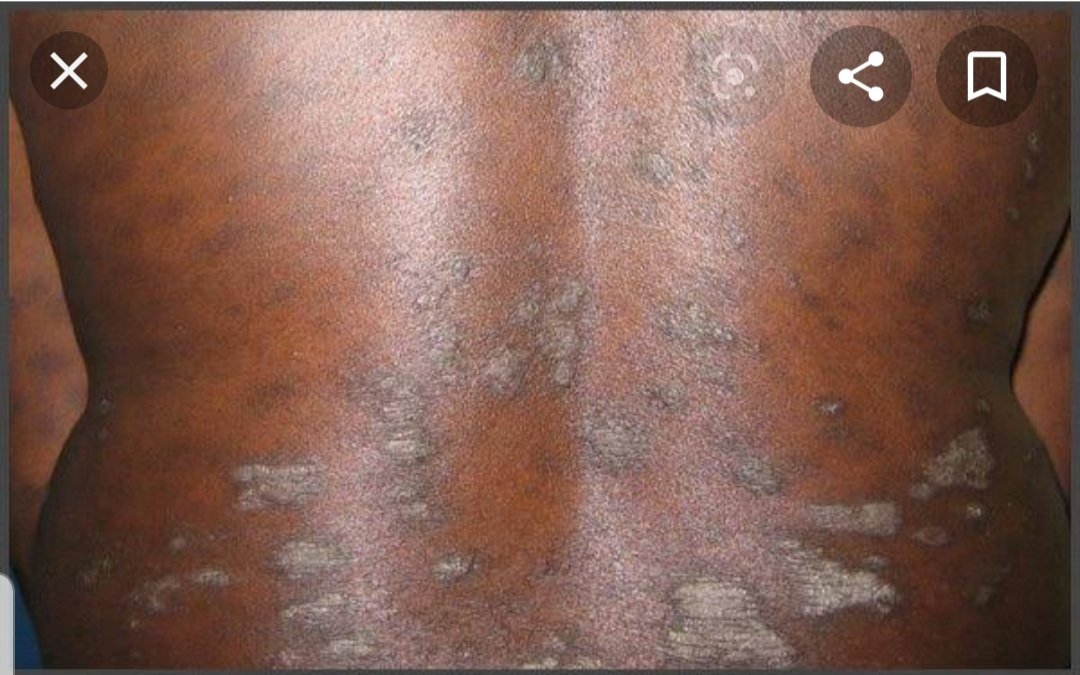
4. History of these scaly lesions in a 47yr old man. Also has hypertension and DM. What is the diagnosis?
Give one differential
Give one differential
5. 6 month old with these asymptomatic lesions. Mother in law brought some leaves.
What is your advice to the parents?
Diagnosis?
What is your advice to the parents?
Diagnosis?

6. Spot diagnosis?

Asymptomatic lesions on the soles of the feet. Emits a putrid smell when he takes off his shoes that have people running for cover.
Diagnosis? Aetiology?
One differential?
Diagnosis? Aetiology?
One differential?

8. Recurrent history of 'boils' in the axilla and groin. Leaves behind sinuses. Has used several drugs. Started after puberty.
Diagnosis?
Diagnosis?

9. History of itching with rashes in this location. Started at age 3. Associated itchy eyes. Mum is asthmatic. Diagnosis?
Most important part of management?
Most important part of management?

10. Lesion noted on the buttocks and tip of the penis. Started initially as erythematous patches. Also noted around the mouth. History of febrile illness with use of some medications called 'akape'.
Diagnosis?
Examples of some implicated agents?
Important aspect of mgt?
Diagnosis?
Examples of some implicated agents?
Important aspect of mgt?

11. Diagnosis?
Started as vesicles that rupture to involve other areas?
Started as vesicles that rupture to involve other areas?

12. Noted since he was born. Family history of lesions in his dad and siblings?
No systemic symptoms.
Diagnosis?
Differential diagnosis?
No systemic symptoms.
Diagnosis?
Differential diagnosis?

Aspiring dermatologists like @SandraGee_
Megalobrainiacs like @ojayfemi .
Please don't let me see you here🙄
To be continued.
Megalobrainiacs like @ojayfemi .
Please don't let me see you here🙄
To be continued.
All questions to be answered at the end of today. Enjoy!
All I know is I'm recruiting residents already. 😂
Will send application letter to successful candidates when I answer the questions at night.
Will send application letter to successful candidates when I answer the questions at night.
Please check under each picture for the answers.
1. Syringomas.
People that said DPNs - Wrong. Those are usually hyperpigmentation stuck on papules. Syringomas here are flesh colored and are tumors of the eccrine sweat glands.
Xanthelasma - No. The medial canthus is spared.
Closest differential- Trichoepithelioma
People that said DPNs - Wrong. Those are usually hyperpigmentation stuck on papules. Syringomas here are flesh colored and are tumors of the eccrine sweat glands.
Xanthelasma - No. The medial canthus is spared.
Closest differential- Trichoepithelioma
2. Papular urticaria. I think this was quite straightforward.
3. Scabies. I intentionally put the posh history of living on Apple island.People think the upper class can't get scabies. Wrong. Close contact with an affected person is all that is needed.
The incubation period is 4 to 6 weeks. Remember to treat all close asymptomatic contacts
The incubation period is 4 to 6 weeks. Remember to treat all close asymptomatic contacts
Psoriasis. Chronic plaque psoriasis. I helped by putting a history of HTN and DM. Someone commented that these are not the typical areas? It can affect any area but commonly extensor surfaces. This doesn't mean it's the only area it affects. Typical lesions of psoriasis
Are described as erythematous well circumscribed scaly plaques with whitish silvery scales. It may not appear so in blacks because of your deeply pigmented skin. Remember to check for scalp and nail involvement.
Differential.. Lichen planus
Differential.. Lichen planus
5. Infantile seborrheic dermatitis
The age is supportive of that. Pityriasis alba rarely starts less than 3yrs. Would have been a great differential.
Pityriasis versicolor starts around puberty.
To leave alone as its self limiting. Usually due to effect of maternal hormones.
The age is supportive of that. Pityriasis alba rarely starts less than 3yrs. Would have been a great differential.
Pityriasis versicolor starts around puberty.
To leave alone as its self limiting. Usually due to effect of maternal hormones.
6. Becker's naevus. Commonly seen in young men. May start around puberty. Saw a lot of people writing vitiligo. The fair skin is the normal skin as it's a Caucasian picture. I thought so many people would get that😊
7. Look at the punched out lesions. Rather than fissure and cracks with scaling seen in Tinea pedis.
This is Pitted Keratolysis. Commonly caused by Corynebacterium minutissimum. And some other bacteria with long names.
Differential- Tinea pedis
This is Pitted Keratolysis. Commonly caused by Corynebacterium minutissimum. And some other bacteria with long names.
Differential- Tinea pedis
8. Hidradenitis suppurativa. Cause unknown. Occurs in otherwise healthy people. Usually starts around puberty. The history of recurrent 'boils' becoming sinuses involving apocrine hair bearing areas (axilla, groin, periareolar area) clinches the diagnosis .
9. Look at the typical areas. Involved in atopic dermatitis. These are chronic ezcematous lesions of atopic dermatitis.
Clincher: Age it started (most cases start under 5)
Associated itchy eyes (vernal conjuctivitis)
Family history of asthma
Counseling (most impt part of mgt)
Clincher: Age it started (most cases start under 5)
Associated itchy eyes (vernal conjuctivitis)
Family history of asthma
Counseling (most impt part of mgt)
10. Fixed drug eruption
Febrile illness with use of akape (cocktail of drugs typically antimalarials, NSAIDs, antibiotics)
Typical locations like perioral and tip of penis.
Implicated drugs: Sulphonamides, NSAIDS, Anticonvulsants
Mgt: Counseling. Never use offending agent again
Febrile illness with use of akape (cocktail of drugs typically antimalarials, NSAIDs, antibiotics)
Typical locations like perioral and tip of penis.
Implicated drugs: Sulphonamides, NSAIDS, Anticonvulsants
Mgt: Counseling. Never use offending agent again
11. Non bullous impetigo. Starts as vesicles that typically rupture to leave behind honey crusts like this.
Contagious. Child may need to be kept away from school while treating for a few days to prevent spreading to others.
Contagious. Child may need to be kept away from school while treating for a few days to prevent spreading to others.
12. Piebaldism.
The history helped. Lesions since birth. Family history in father and siblings.
No systemic symptoms.
Vitiligo is a differential but history rules it out. Vitiligo is acquired and not from birth.
The history helped. Lesions since birth. Family history in father and siblings.
No systemic symptoms.
Vitiligo is a differential but history rules it out. Vitiligo is acquired and not from birth.













