I've shared concerns about @onemedical and their commercial strategy before; new data illustrates the issue.
TL;DR:
- In SF, some ONEM visit prices run 350 - 400% of Medicare
- Employers should be cautious. Proactive primary care can cut costs, but this is not the way.
1/n
TL;DR:
- In SF, some ONEM visit prices run 350 - 400% of Medicare
- Employers should be cautious. Proactive primary care can cut costs, but this is not the way.
1/n
Two points for context:
1) Evidence suggests that high-performing PCPs can save $$, even in the commercial population.
E.g. @Mass_HPC, finds risk-adjusted cost deltas up to $1,500 PMPY across medical groups, via referral patterns (i.e. secondary care prices) and low-value care
1) Evidence suggests that high-performing PCPs can save $$, even in the commercial population.
E.g. @Mass_HPC, finds risk-adjusted cost deltas up to $1,500 PMPY across medical groups, via referral patterns (i.e. secondary care prices) and low-value care
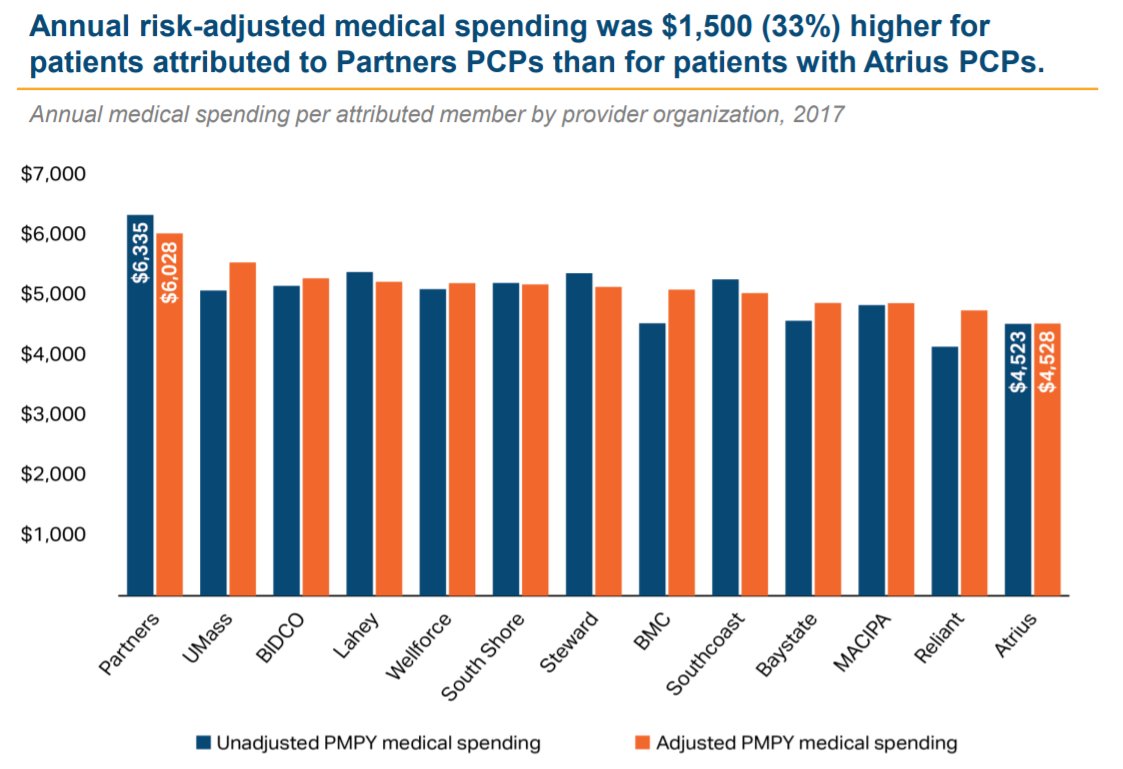
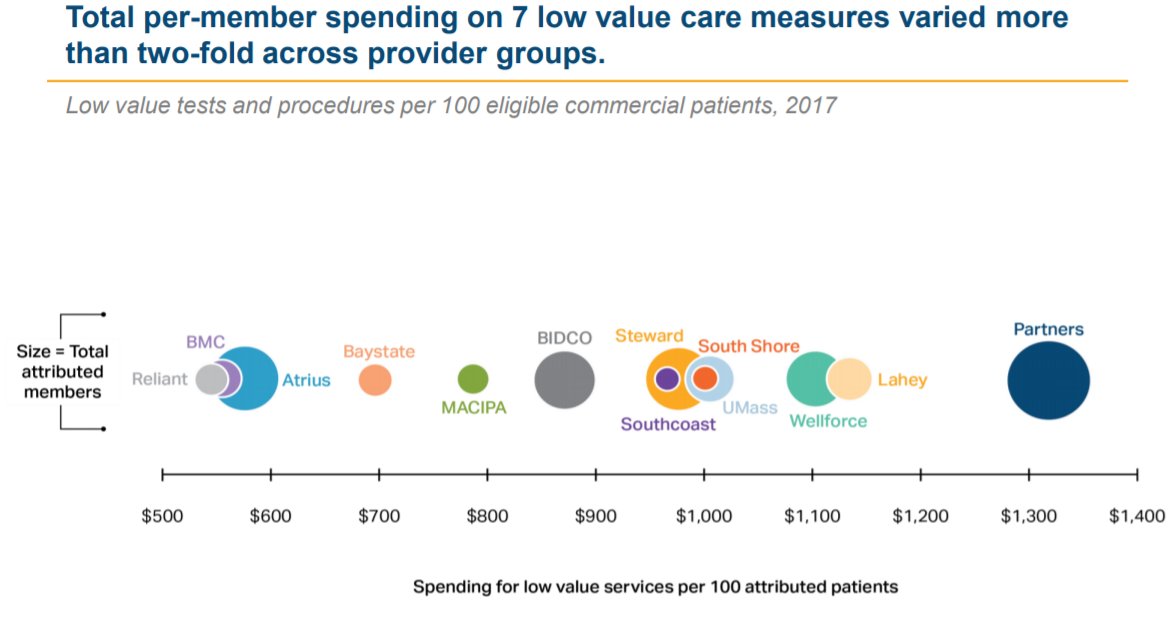
2) As noted elsewhere, One Medical's strategy seems to rely heavily on price arbitrage - i.e. billing under the umbrella of a higher-priced health system - which would be to the clear detriment of employers who pay these claims.
More on that here:
More on that here:
The new data that caught my eye comes from an EOB after a routine annual checkup in December, and a follow-up conversation with ONEM staff to understand exactly what codes they submitted.
In short, all-in cost for this one <15-min visit was $460, plus $138 for routine lab tests.
In short, all-in cost for this one <15-min visit was $460, plus $138 for routine lab tests.
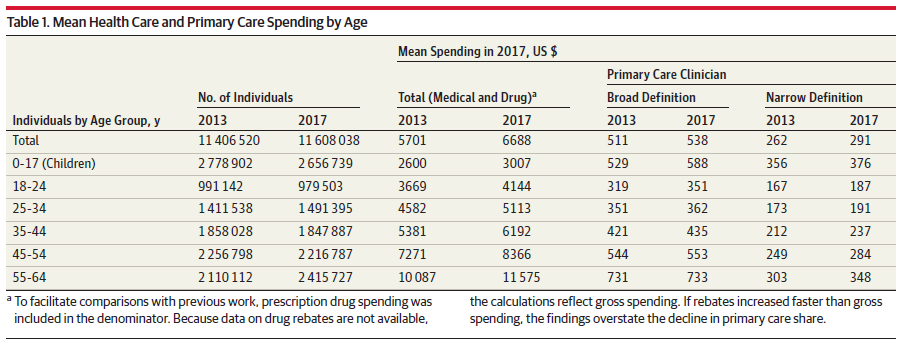
This is a bit startling, but that one visit, then, exceeds the typical ANNUAL cost for *all primary care* - on a fairly broad definition - for a commercial patient in this age range. To be clear, that is before the cost of the lab work itself.
Receipts (h/t to @HealthCostInst):
Receipts (h/t to @HealthCostInst):
Arguably even more eye-catching when you unpack this. ONEM billed two codes here:
- 99395, which is a routine preventive medicine visit for an established patient.
- 36415, for the in-office blood draw
Note: LabCorp billed the actual tests, at reasonable-ish prices.
- 99395, which is a routine preventive medicine visit for an established patient.
- 36415, for the in-office blood draw
Note: LabCorp billed the actual tests, at reasonable-ish prices.

For the first (99395), a Medicare Advantage plan would reimburse something like $130. Kaiser Permanente's cash price (for HDHP members) in Northern California would be somewhere btwn $85 and $220, depending on how they coded it.
So...ONEM is pricing this at ~350% of Medicare.
So...ONEM is pricing this at ~350% of Medicare.

Note: Since I'm trying to adopt "% of Wal-Mart" as the new pricing standard, I will just note that WMT charges $30 for an adult annual checkup at their new centers in Georgia. So, One Medical's pricing would appear to be...
[checks notes]
1,500% of Wal-Mart.
[checks notes]
1,500% of Wal-Mart.
Then there is the $11.73 venipuncture...
Debatable to reimburse this at all. Per Anthem, for example, 36415 is not eligible for separate reimbursement on top of a routine E/M ofc visit.
In any case, Medicare pays $3, (its 5 mins of phlebotomist time). So... ~400% of Medicare.
Debatable to reimburse this at all. Per Anthem, for example, 36415 is not eligible for separate reimbursement on top of a routine E/M ofc visit.
In any case, Medicare pays $3, (its 5 mins of phlebotomist time). So... ~400% of Medicare.
All of this is pretty extreme.
Feels like upcoding - given the lack of a problem, Dx or preventive counseling, it arguably should be coded as 99212/3.
And the price is just inexplicably high. Bay Area AMCs (UCSF, Stanford etc) charge 200-300% of Medicare for inpatient care.
Feels like upcoding - given the lack of a problem, Dx or preventive counseling, it arguably should be coded as 99212/3.
And the price is just inexplicably high. Bay Area AMCs (UCSF, Stanford etc) charge 200-300% of Medicare for inpatient care.
Challenge for employers is just...the math.
At prices this high, sending staff to ONEM could double or triple their primary care spend (assuming ~2.5 visits PMPY). And then, referral relationships w/ high-cost secondary care will eliminate one of the best savings vectors.
At prices this high, sending staff to ONEM could double or triple their primary care spend (assuming ~2.5 visits PMPY). And then, referral relationships w/ high-cost secondary care will eliminate one of the best savings vectors.
That leaves you pretty dependent on avoiding ED visits.
But if the baseline ED utilization is 0.2 - 0.3 ED visits PMPY at, say, $1,400 a pop, there are just not enough avoidable ED visits to offset the additional outlays on high-priced primary care.
But if the baseline ED utilization is 0.2 - 0.3 ED visits PMPY at, say, $1,400 a pop, there are just not enough avoidable ED visits to offset the additional outlays on high-priced primary care.
Finally, because ONEM remains primarily FFS, w/ gross margins well north of 50% on a $460 visit, they are highly-incented to maximize billable visit volume.
All-in, while I'm a fan of investing in primary care, it is hard to see how this revenue model works for employers. /n
All-in, while I'm a fan of investing in primary care, it is hard to see how this revenue model works for employers. /n
Addendum:
Today's One Medical marketing email really captures the result of high visit prices & fee-for-service.
Members are invited to:
A 4-week "stress management program"...
...led by "holistic health providers"...
...and "billed to your insurance as a medical visit."
Today's One Medical marketing email really captures the result of high visit prices & fee-for-service.
Members are invited to:
A 4-week "stress management program"...
...led by "holistic health providers"...
...and "billed to your insurance as a medical visit."