
I was feeling overwhelmed by all the laypress articles about #moralinjury and #burnout in frontline health care workers during #Covid_19 so I decided to do a deep dive into the literature on the mental health of workers during pandemics.
Here's what I found. #thread
1/
Here's what I found. #thread
1/
Seriously, so many laypress articles.
What evidence do we have on this, and further, what evidence do we have on strategies that mitigate these mental health issues in health care workers?
I presented these data the @UChicagoMed @UCCancerCenter grand rounds last week.
2/
What evidence do we have on this, and further, what evidence do we have on strategies that mitigate these mental health issues in health care workers?
I presented these data the @UChicagoMed @UCCancerCenter grand rounds last week.
2/
@UChicagoMed @UCCancerCenter But first, some definitions to set the stage:
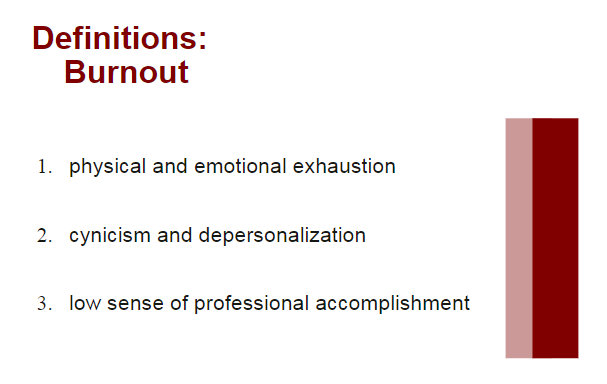
Burnout, initially described by Dr. Maslach as the prolonged physical and psychological exhaustion related to a person's work. Not specific to medicine, although the definition has been honed for medicine (see slide). #burnout
3/x
Burnout, initially described by Dr. Maslach as the prolonged physical and psychological exhaustion related to a person's work. Not specific to medicine, although the definition has been honed for medicine (see slide). #burnout
3/x
So, researchers who described burnout realized that the mental health phenomenon in health care workers was different, because it involved trauma:
Enter: compassion fatigue (= burnout + secondary traumatic stress). Better definition for what health care workers experience.
5/
Enter: compassion fatigue (= burnout + secondary traumatic stress). Better definition for what health care workers experience.
5/
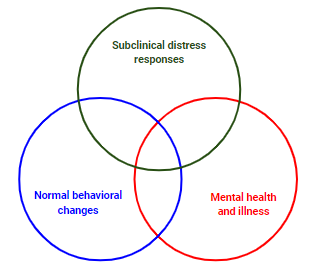
Super important to note: not all trauma (primary or secondary) to health care workers results in long-term mental health sequelae.
There is spectrum of responses, the majority normal, less which are subclinical (like compassion fatigue), and even less with frank PTSD.
6/
There is spectrum of responses, the majority normal, less which are subclinical (like compassion fatigue), and even less with frank PTSD.
6/
So, how does #moralinjury fit into all this?
Short story: it's complicated.
Long story: keep following the #thread. #burnout #ptsd
7/
Short story: it's complicated.
Long story: keep following the #thread. #burnout #ptsd
7/
Moral injury was first described in the military, specifically by Dr. Jonathan Shay in 1998 after studying Vietnam era veterans.
Initial definition: “a betrayal of what’s right, by someone who holds legitimate authority, in a high-stakes situation.” #moralinjury
8/
Initial definition: “a betrayal of what’s right, by someone who holds legitimate authority, in a high-stakes situation.” #moralinjury
8/
Fast forward to 2018 and Dr. Wendy Dean's laypress article in @statnews: "Physicians aren’t ‘burning out.’ They’re suffering from moral injury"
statnews.com/2018/07/26/phy…
In short: #burnout doesn't reflect systemic pressures that affect mental health of health care workers.
9/
statnews.com/2018/07/26/phy…
In short: #burnout doesn't reflect systemic pressures that affect mental health of health care workers.
9/
In a follow-up academic piece, Dr. Dean defines #moralinjury in health care workers as follows:
"the challenge of simultaneously knowing what care patients need but being unable to provide it due to constraints that are beyond our control"
ncbi.nlm.nih.gov/pmc/articles/P…
10/
"the challenge of simultaneously knowing what care patients need but being unable to provide it due to constraints that are beyond our control"
ncbi.nlm.nih.gov/pmc/articles/P…
10/
This #moralinjury definition obviously applies to #COVID19 era health care workers: we have a moral duty to provide care, and we cannot provide that care to the best of our abilities due to systemic issues that we cannot control.
Theoretically, this makes sense. However...
11/
Theoretically, this makes sense. However...
11/
...moral injury has not been systematically studied in health care workers. We don't have any validated instruments like we do in #burnout or #compassionfatigue.
Further, which comes first? Moral injury --> compassion fatigue? Burnout --> moral injury? How are they related?
12/
Further, which comes first? Moral injury --> compassion fatigue? Burnout --> moral injury? How are they related?
12/
So, we don't evidence for #moralinjury. However, it turns out there is a great base of literature studying #burnout, acute and chronic stress, and #PTSD in health care workers in other pandemics.
Now, we transition this #thread to historical precedents, specifically SARS.
13/
Now, we transition this #thread to historical precedents, specifically SARS.
13/
SARS presents a comparable model to #COVID19 in studying mental health effects on health care workers.
Although only ~8000 cases worldwide of #SARS back in 2003, many similarities in transmission, high nosocomial spread, and use of #quarantine in China and Canada.
14/
Although only ~8000 cases worldwide of #SARS back in 2003, many similarities in transmission, high nosocomial spread, and use of #quarantine in China and Canada.
14/
Next up, I want to present a few of the larger studies that specifically looked at mental health in health care workers during SARS. Will include links to the original papers as well as my slides.
#covid4mds #moralinjury #SARSCoV2 #foamcovid
15/
#covid4mds #moralinjury #SARSCoV2 #foamcovid
15/
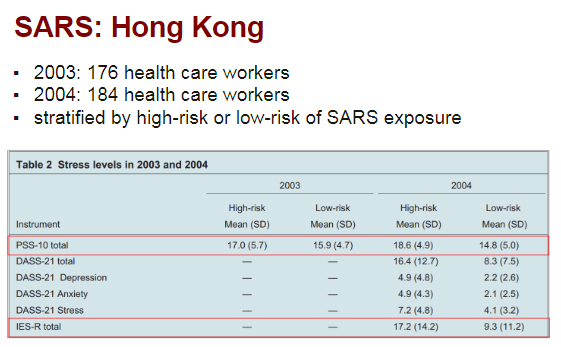
First, study in Hong Kong of HC workers in 2003 during outbreak and 1 year later.
- High-risk and low-risk workers both had high acute and chronic stress.
- Chronic stress increased 1 year later in high-risk workers.
- #PTSD higher in high-risk.
ncbi.nlm.nih.gov/pubmed/17500305
16/
- High-risk and low-risk workers both had high acute and chronic stress.
- Chronic stress increased 1 year later in high-risk workers.
- #PTSD higher in high-risk.
ncbi.nlm.nih.gov/pubmed/17500305
16/
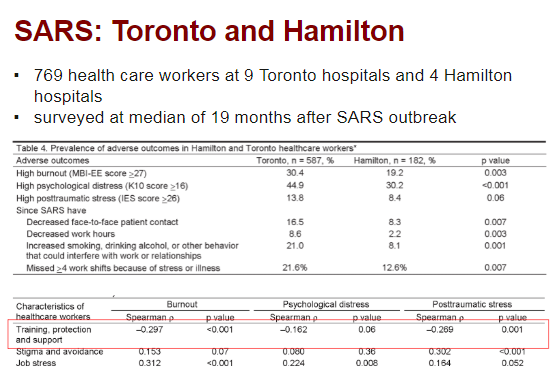
Next study in Toronto with SARS cases, using Hamilton as control with no SARS cases but same infection control measures.
- High #burnout & #PTSD >1 year after outbreak, worse if exposed to SARS pts.
- Adequate PPE and support = less burnout & PTSD.
ncbi.nlm.nih.gov/pubmed/17326946
17/
- High #burnout & #PTSD >1 year after outbreak, worse if exposed to SARS pts.
- Adequate PPE and support = less burnout & PTSD.
ncbi.nlm.nih.gov/pubmed/17326946
17/
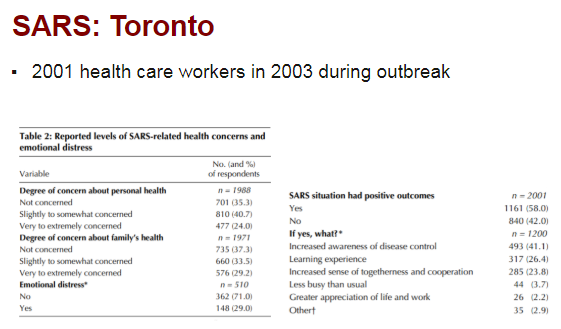
Final study in Toronto of HC workers during 2003 #SARS:
- 30% acute emotional distress in health care workers.
- 45% nurses, 33% allied HC professionals, 17% physicians with acute distress.
- 58% felt SARS has positive outcomes (see slide).
ncbi.nlm.nih.gov/pubmed/14993174
18/
- 30% acute emotional distress in health care workers.
- 45% nurses, 33% allied HC professionals, 17% physicians with acute distress.
- 58% felt SARS has positive outcomes (see slide).
ncbi.nlm.nih.gov/pubmed/14993174
18/
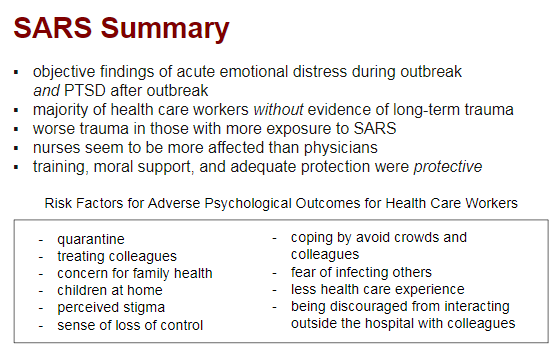
Another big point to take away from 2003 #SARS literature:
Adequate training, PPE, and feeling of support were PROTECTIVE of poor mental health outcomes for health care workers.
The first inkling from the literature that structural / organizational efforts have efficacy.
20/
Adequate training, PPE, and feeling of support were PROTECTIVE of poor mental health outcomes for health care workers.
The first inkling from the literature that structural / organizational efforts have efficacy.
20/
So, what did we learn from SARS?
First, a good thing: the majority of health care workers *just get better* with respect to both acute and chronic stress.
However, chronic stress leads to attrition out of patient care (see Toronto/Hamilton study in #thread).
21/
First, a good thing: the majority of health care workers *just get better* with respect to both acute and chronic stress.
However, chronic stress leads to attrition out of patient care (see Toronto/Hamilton study in #thread).
21/

However, #COVID19 is obviously *very different* from #SARS.
Much more widespread, more limitations on resources for health care worker protection AND patient care (#PPE, #ventilatorshortage) --> potentially more moral injury?
This needs research in current #pandemic.
22/
Much more widespread, more limitations on resources for health care worker protection AND patient care (#PPE, #ventilatorshortage) --> potentially more moral injury?
This needs research in current #pandemic.
22/
So, we know from #SARS research that health care workers experience #burnout and
#mentalillness during and after pandemics.
My next goal was to find evidence-based strategies for mitigation of these moral and emotional insults.
The #thread continues with that research.
23/
#mentalillness during and after pandemics.
My next goal was to find evidence-based strategies for mitigation of these moral and emotional insults.
The #thread continues with that research.
23/
First, I want to propose these psychological phases of HC workers during pandemics (modified from work by Chong et al).
I overlaid the evidence-based frameworks on top.
Remember: different ares will be at different points on this timeline.
cambridge.org/core/services/…
24/
I overlaid the evidence-based frameworks on top.
Remember: different ares will be at different points on this timeline.
cambridge.org/core/services/…
24/
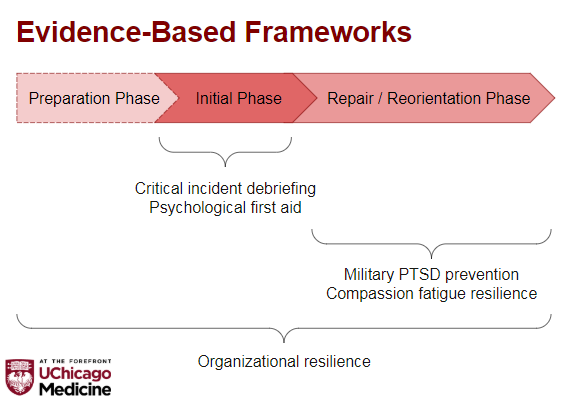
So, let's start with critical incident debriefing, a popular means of managing acute trauma in first responders & health care workers.
Long story short: super controversial, and meta-analyses have showed that it may actually INCREASE risk of #PTSD.
jenonline.org/article/S0099-…
25/
Long story short: super controversial, and meta-analyses have showed that it may actually INCREASE risk of #PTSD.
jenonline.org/article/S0099-…
25/
Rather than critical incident debriefing, which pathologizes normal emotional responses to trauma, psychological first aid embraces those emotional responses as normal and provides health care workers with the communal support that research demonstrates is protective.
27/
27/
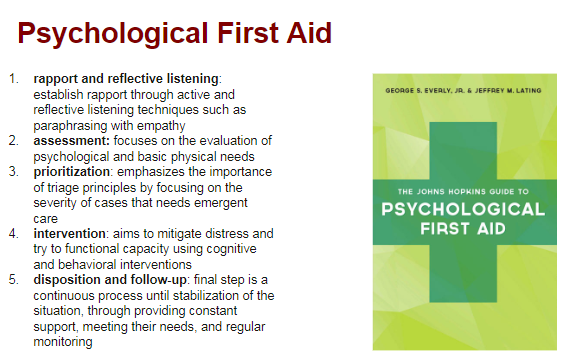
Psychological first aid is endorsed by @WHO, @APAPsychiatric and @NIMHgov as evidence-based strategy for management of acute trauma for first responders & health care workers.
Anyone can learn to do it, too! Not just mental health workers: apa.org/practice/progr…
28/
Anyone can learn to do it, too! Not just mental health workers: apa.org/practice/progr…
28/
Based on initial work in Vietnam field hospital nurses, and later in deployed HC workers in Iraq, we know that deployment results in worse #PTSD & #depression.
However, important to note that *perceived threat of harm* predicts development of PTSD rather than just exposure.
30/
However, important to note that *perceived threat of harm* predicts development of PTSD rather than just exposure.
30/
... reducing *perceived threat* to health care workers during a #pandemic should protect their #mentalhealth.
Adding to this assertion is the finding in military literature that strong, compassionate leadership is also *protective* against development of #PTSD.
32/
Adding to this assertion is the finding in military literature that strong, compassionate leadership is also *protective* against development of #PTSD.
32/
Another evidence-based framework specifically focuses on #compassionfatigue.
The Accelerated Recovery Program, developed in the 1990s, is a group CBT-approach to reducing CF & #PTSD, with efficacy demonstrated in nurses.
However, has not been studied in epidemic setting.
33/
The Accelerated Recovery Program, developed in the 1990s, is a group CBT-approach to reducing CF & #PTSD, with efficacy demonstrated in nurses.
However, has not been studied in epidemic setting.
33/
The final framework I want to discuss is arguably the most important: organizational resilience.
I know this #thread is getting long, but I want to really spend some time on the evidence that supports organizational interventions in protecting HC worker mental health.
34/
I know this #thread is getting long, but I want to really spend some time on the evidence that supports organizational interventions in protecting HC worker mental health.
34/
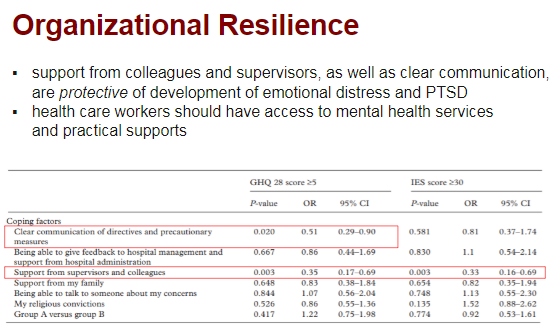
"Organizational resilience" is a term coined Dr. Maunder based on mental health of HC workers during #SARS.
It refers to an system-wide approach that provides for *all* of the needs of health care workers (mental AND physical) during crises.
ncbi.nlm.nih.gov/pmc/articles/P…
35/
It refers to an system-wide approach that provides for *all* of the needs of health care workers (mental AND physical) during crises.
ncbi.nlm.nih.gov/pmc/articles/P…
35/
Evidence from SARS (see slide) suggests that 1) clear communication and 2) support from supervisors & colleagues was protective of generalized distress and #PTSD in HC workers.
This adds to the existing military literature that leadership is protective against PTSD.
36/
This adds to the existing military literature that leadership is protective against PTSD.
36/
I hope I'm making a clear argument that compassionate leadership and adequate training & support of health care workers has been demonstrated in the literature to protect their mental health in previous SARS outbreak and military literature.
But, that's not all. #thread
37/
But, that's not all. #thread
37/
Organizational resilience also involves providing for the *physical* and *practical* needs of health care workers, including:
- adequate #PPE
- hazard/overtime pay
- housing/childcare support
- access to groceries/food
- scrubs
- timely mental health services if needed
38/
- adequate #PPE
- hazard/overtime pay
- housing/childcare support
- access to groceries/food
- scrubs
- timely mental health services if needed
38/
Now, the most important conclusion from this whole #thread:
ORGANIZATION-LEVEL SUPPORT OF HEALTH CARE WORKERS IS A MENTAL HEALTH INTERVENTION.
The literature I cited supports this assertion. Yes, individual-level #burnout and #compassionfatigue tools are important, but...
39/
ORGANIZATION-LEVEL SUPPORT OF HEALTH CARE WORKERS IS A MENTAL HEALTH INTERVENTION.
The literature I cited supports this assertion. Yes, individual-level #burnout and #compassionfatigue tools are important, but...
39/
...a comprehensive (not siloed!) approach to addressing the mental, social, and physical needs of health care workers is critical in protecting their mental health in this unprecedented #COVID19 pandemic.'
How #moralinjury plays into this is completely unknown.
40/
How #moralinjury plays into this is completely unknown.
40/
I few of my conclusions from this literature review on the attached slide.
Modern health care has never seen this type of trauma before, and dedicated study of #moralinjury, as well as #burnout, #compassionfatigue and #PTSD in health care workers is warranted.
41/
Modern health care has never seen this type of trauma before, and dedicated study of #moralinjury, as well as #burnout, #compassionfatigue and #PTSD in health care workers is warranted.
41/
areas*. Sorry, typing too fast!

