
,
27 tweets,
13 min read
Read on Twitter
(Thread)
I’m going to discuss how physician payment rates in the US are set and suggest a reason why #primarycare is poorly valued from a salary standpoint in the U.S. I’ll also suggest how anyone interested can work to improve payment for #primarycare.
1/
I’m going to discuss how physician payment rates in the US are set and suggest a reason why #primarycare is poorly valued from a salary standpoint in the U.S. I’ll also suggest how anyone interested can work to improve payment for #primarycare.
1/
I am targeting younger physicians and medical students - this may be too simplistic for some, and go into the weeds too much for others. But the whippersnappers are the ones that are more likely to lead change, and so that is the audience here.
2/
2/
Disclaimer: I am an academic #pulmcc physician, not a #primarycare physician. So I’m in a procedure-heavy specialty. I'm also not an expert in health policy, so feel free to gently correct anything that seems off.
3/
3/
This thread was inspired by this study in JAMA that correlates #primarycare physician density with lower population mortality- every additional 10 #primarycare physicians-> 51.5 day increase in life expectancy. The data are pretty impressive.
bit.ly/2BMEvMS
4/
bit.ly/2BMEvMS
4/
Some have suggested policy changes to encourage careers in #primarycare. Surprisingly, there are little data looking at the role of salary in specialty selection, but it seems absurd to think that salary is not a major driver of specialty selection.
5/
5/
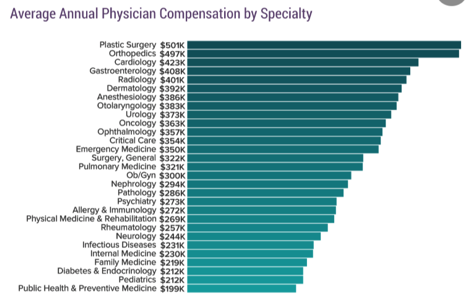
And specialties that are procedure-based make far more than specialties that require more thinking than doing. #Primarycare obviously fits into the “thinking” category here.
7/
7/
Is it just that plastic surgeons work a LOT HARDER than those in #primarycare? Not according to this study from JAMA in 2011- these data suggest that the average plastic surgeon, who makes 228% more, works less hours than the average family practice MD. bit.ly/2STIZvO8/
8/
8/

So, then how is it determined that a plastic surgeon’s time is worth more than an FP (I’m picking on them arbitrarily- sorry to my colleagues in those specialties)? In order to understand this, one must journey down the RVU rabbithole. It won’t take too long.
9/
9/
RVUs, Relative Value Units, are the measure of value for work- when a claim is submitted for payment, it is submitted as a Current Procedural Terminology (CPT) code, and each CPT code is assigned a certain number of RVUs that determines what will be paid to the provider. 10/
The RVU system was developed in the Omnibus budget reconciliation act of 1989. The @amermedicalassn owns the copyright for CPT codes (and they are its biggest source of revenue). The CPT system was developed in 1966 to focus on- you guessed it- surgical procedures.
11/
11/
You can see more about RVUs in this 2-pager from the National Health Policy Forum (which served government from 1972-2016, when it was shuttered). It has this graphic, which highlights the “procedure-heavy” nature of the RVU system. bit.ly/2tybDU8 12/

Many physicians are then paid on a certain dollar-per-RVU basis. So RVUs determine how much physicians get paid for doing certain CPT codes. You can explore RVU values using this RVU calculator, provided by @aapcstaff. bit.ly/2GSELNM
12/
12/
Office visits are paid as "evaluation and management", or E/M codes. The most common E/M codes are 99201-99205 (new patients) and 99211-99215.
13/
13/
E/M codes fall behind procedural codes- A screening colonoscopy takes ~25 minutes and generates 3.26 RVUs. A similarly timed return visit generates 1.5 RVUs. One can argue there should be “hazard pay” for procedural risk, and I agree with this. Is this time worth 117% more?
14/
14/
One can easily see how incentives make it hard to justify taking the time to counsel a patient on the risks and benefits of a procedure they maybe shouldn’t have rather than just doing it.
15/
15/
So, if physician work-> CPT code-> RVU-> payment amount, then how is the RVU value determined? THIS IS WHERE THIS THREAD GETS IMPORTANT.
17/
17/
RVUs values are assigned by @CMSGov, who relies HEAVILY on the @amermedicalassn Specialty Society Relative Value Scale Update Committee [RUC, which rhymes with truck]. Historically, @cmsgov has accepted the RUC’s recommendations ~ 90% of the time.
18/
18/
The RUC is comprised of 31 members. Currently only 4 of these 31 members represent a #primarycare specialty. You can find the makeup and specialties of the members here: bit.ly/2EnsC1E
19/
19/
The RUC has focused on improving reimbursement for primary care- you can see their efforts in this document: bit.ly/2SVV7wp. But E/M reimbursement still lags, making #primarycare far underpaid compared to other specialties.
20/
20/
From what I can tell, the last time the RUC recommended a large change to the E/M RVUs was 2007. (I had to pull these data from the federal register, 71(125):37188.) So it is not as though these rates haven’t increased- this was a significant change in 2007. 21/

Sidenote: @cmsgov has a new proposed rule that would dramatically change the RVU structure of E/M visits- you can learn more here: bit.ly/2BJiEWH
22/
22/
I WOULD ARGUE THAT THE MAKEUP OF THE RUC AND ITS RECOMMENDATIONS TO @CMSGOV HAS MORE INFLUENCE ON INDIVIDUAL CHOICES REGARDING PHYSICIAN SPECIALTY SELECTION THAN ANY OTHER.
23/
23/
I would further argue that the RUC should have:
1.More #primarycare representation equitably represent physician work in the US.
2.Include economists and public health experts to help create incentives to move the physician workforce in a measured way based upon need.
24/
1.More #primarycare representation equitably represent physician work in the US.
2.Include economists and public health experts to help create incentives to move the physician workforce in a measured way based upon need.
24/
So- policy change that would incentivize more #primarycare would come through both @cmsgov and @amermedicalassn. Efforts should be aimed at pressuring @amermedicalassn to change the RUC to include more primary care, public health experts, and economists in its RVU decisions. 25/
You can read more about this at slate.com/news-and-polit… and well.blogs.nytimes.com/2011/09/22/how…
And here is a recent article that highlights the issues with the RVU system when it comes to dialysis: “Low reimbursement for monthly office visits to supervise conservative management might doom a practice financially.”
nytimes.com/2019/02/15/hea…
nytimes.com/2019/02/15/hea…














