

3/20
Therapies mixing the best of both worlds, have being present for a while
💥Smart people delivering what´s NEEDED with the tools AVAILABLE
💥What´s NEEDED?: Replace renal function on unstable critically ill patients without actually killing the patient in the process
Therapies mixing the best of both worlds, have being present for a while
💥Smart people delivering what´s NEEDED with the tools AVAILABLE
💥What´s NEEDED?: Replace renal function on unstable critically ill patients without actually killing the patient in the process
4/20
🤔 But why so much confusion with these mixed therapies?
A: The different strategies and nomenclature used in literature make difficult to:
1. Compare it with CRRT
2. Evaluate outcomes and complications as a unique therapy
3. Establish a standard dose
🤔 But why so much confusion with these mixed therapies?
A: The different strategies and nomenclature used in literature make difficult to:
1. Compare it with CRRT
2. Evaluate outcomes and complications as a unique therapy
3. Establish a standard dose
6/20
Considering this☝️, 2 interchangeable terms exist:
⚡HYBRID: Word to define MIXED
⚡PIRRT: Prolonged Intermittent Renal Replacement Therapy
We then, can divide them in therapies that:
1. Try to be more like CRRT (SLED, SLED-f)
2. Try to be more like iHD (AVVH, SHIFT)
Considering this☝️, 2 interchangeable terms exist:
⚡HYBRID: Word to define MIXED
⚡PIRRT: Prolonged Intermittent Renal Replacement Therapy
We then, can divide them in therapies that:
1. Try to be more like CRRT (SLED, SLED-f)
2. Try to be more like iHD (AVVH, SHIFT)

7/20
⚡️iHD machine trying to be #CRRT⚡️
S-L-E-D
Sustained Low Efficiency Dialysis
🔥From the NAME we know:
1. Sustained (More time but not continuous)
2. Low efficiency (Low Qd and Qb, ⬇ml/min)
3. Dialysis (Diffusion)
⚡️iHD machine trying to be #CRRT⚡️
S-L-E-D
Sustained Low Efficiency Dialysis
🔥From the NAME we know:
1. Sustained (More time but not continuous)
2. Low efficiency (Low Qd and Qb, ⬇ml/min)
3. Dialysis (Diffusion)
8/20
How SLED is performed?
⚡️iHD Machine
⚡️Qb: 200 ml/min
⚡️Qd: 100-200 ml/min
🔥(this is the most challenging parameter to costume on an iHD machine, some machines need software adjustments or home made by-pass systems🔥
⚡️Time 6-12 hours
⚡️Days: 6
Machines adjustments
How SLED is performed?
⚡️iHD Machine
⚡️Qb: 200 ml/min
⚡️Qd: 100-200 ml/min
🔥(this is the most challenging parameter to costume on an iHD machine, some machines need software adjustments or home made by-pass systems🔥
⚡️Time 6-12 hours
⚡️Days: 6
Machines adjustments

9/20
How to DOSE a SLED?
❌NO answer to this question
✅Equivalent clearance to other therapies will be logical
Minimal recommended dose in AKI:
⚡️iHD--> 3.9 weekly KtV
⚡️CRRT-> 20-25 ml/kg/hr
How can we translate this to a SLED:
Get your #adequators and calculators
How to DOSE a SLED?
❌NO answer to this question
✅Equivalent clearance to other therapies will be logical
Minimal recommended dose in AKI:
⚡️iHD--> 3.9 weekly KtV
⚡️CRRT-> 20-25 ml/kg/hr
How can we translate this to a SLED:
Get your #adequators and calculators
10/20
3.9 Weekly KtV will be achieved with 6 sessions per week that obtain a 60% URR or a 0.9 eKTV (Img1)
The time needed to achieve it, will depend on efficiency parameters, Qd, Qb:
🔥iHD:QB 300/ Qd 500/->T needed 3 hrs (Img 2)
🔥SLED:QB 200/Qd 100/->T needed 7 hrs (Img 3)
3.9 Weekly KtV will be achieved with 6 sessions per week that obtain a 60% URR or a 0.9 eKTV (Img1)
The time needed to achieve it, will depend on efficiency parameters, Qd, Qb:
🔥iHD:QB 300/ Qd 500/->T needed 3 hrs (Img 2)
🔥SLED:QB 200/Qd 100/->T needed 7 hrs (Img 3)



11/20
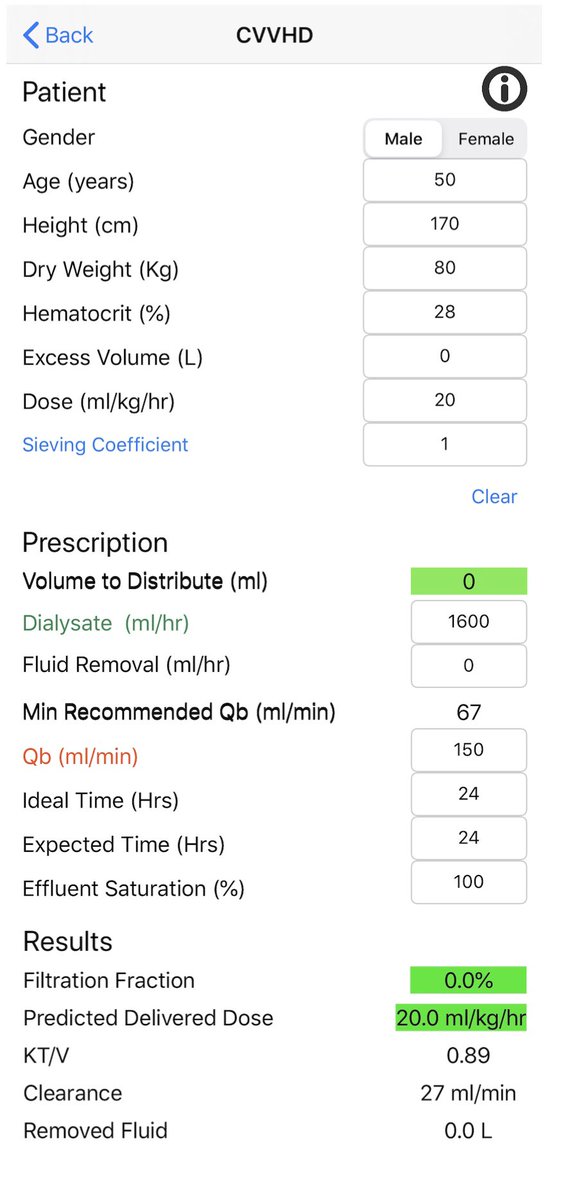
20 ml/kg/hr for 24 hours in a 80 kg male will be equivalent to an eKT/V of 0.9 (Img1)
80 x 20 = 1600
1600 x 24h = 38.4 L
-Urea V = 41 L
38.4/41 = 0.9
eKT/V = 0.9
How much time needed?
🔥CRRT: QB 150/ Qd 26 ->Time 24 h (Img2)
🔥SLED: QB 200/Qd 100 ->Time 7 h (img3)
20 ml/kg/hr for 24 hours in a 80 kg male will be equivalent to an eKT/V of 0.9 (Img1)
80 x 20 = 1600
1600 x 24h = 38.4 L
-Urea V = 41 L
38.4/41 = 0.9
eKT/V = 0.9
How much time needed?
🔥CRRT: QB 150/ Qd 26 ->Time 24 h (Img2)
🔥SLED: QB 200/Qd 100 ->Time 7 h (img3)


12/20
⚡️CRRT machine trying to be #iHD⚡️
A-V-V-H
Accelerated V V Hemofiltration
🔥From the NAME we know
1. Accelerated (Not continuos, delivers a dose in less time, needs better efficiency)
2. VV Hemofiltration (Convection)
⚡️CRRT machine trying to be #iHD⚡️
A-V-V-H
Accelerated V V Hemofiltration
🔥From the NAME we know
1. Accelerated (Not continuos, delivers a dose in less time, needs better efficiency)
2. VV Hemofiltration (Convection)
13/20
🔥How AVVH is performed?
⚡️CRRT machine in CVVH mode
⚡️Qb: 350 ml/min
⚡️Qr:PRE dilution: 50 ml/kg/hr/ 4L/hr /66 ml/min
⚡️Time: 9 hours
⚡️Days: 6
doi.org/10.1053/j.ajkd…
🔥How AVVH is performed?
⚡️CRRT machine in CVVH mode
⚡️Qb: 350 ml/min
⚡️Qr:PRE dilution: 50 ml/kg/hr/ 4L/hr /66 ml/min
⚡️Time: 9 hours
⚡️Days: 6
doi.org/10.1053/j.ajkd…
14/20
🔥Lets calculate how will this therapy will perform
80 x 50 = 4L
4x 9h = 36 L
-Urea V = 41 L
36/41 = 0.9
KT/V= 0.9
🤭But wait, remember we are using PRE, that will dilute solutes
🤔How much? 21% (other tweetorial)
36 *(1-0.21)= 28.4
28.4/41= 0.7
KT/V= 0.7
🔥Lets calculate how will this therapy will perform
80 x 50 = 4L
4x 9h = 36 L
-Urea V = 41 L
36/41 = 0.9
KT/V= 0.9
🤭But wait, remember we are using PRE, that will dilute solutes
🤔How much? 21% (other tweetorial)
36 *(1-0.21)= 28.4
28.4/41= 0.7
KT/V= 0.7
16/20
🤔 CRRT or PIRRT/HYBRID?
Meta- analysis 2015
7 RCT & 10 observational
-RCT: no difference in mortality, kidney recovery, fluid removal, or UCI days
-Observational: less mortality in PIRRT group (Selection bias)
doi.org/10.1053/j.ajkd…
🤔 CRRT or PIRRT/HYBRID?
Meta- analysis 2015
7 RCT & 10 observational
-RCT: no difference in mortality, kidney recovery, fluid removal, or UCI days
-Observational: less mortality in PIRRT group (Selection bias)
doi.org/10.1053/j.ajkd…
17/20
The mayor PROBLEM with HYBRID:
DOSE & TIMING OF MEDICATION
-IHD: K during a short time of day, dosing can come after (lots of data)
-CRRT: K is continuos so dosing can be some how predictable
-SLED: K is not continuous but not a short time of the day (Also no data)
The mayor PROBLEM with HYBRID:
DOSE & TIMING OF MEDICATION
-IHD: K during a short time of day, dosing can come after (lots of data)
-CRRT: K is continuos so dosing can be some how predictable
-SLED: K is not continuous but not a short time of the day (Also no data)
18/20
🔥 When to Choose PIRRT/HYBRID ?
1. Need to perform a therapy with the goals of a CRRT or IHD but the respective machine is not available
2. Transition from CRRT to iHD
3. Nocturnal therapy allowing machine independence during the day for procedures or studies
🔥 When to Choose PIRRT/HYBRID ?
1. Need to perform a therapy with the goals of a CRRT or IHD but the respective machine is not available
2. Transition from CRRT to iHD
3. Nocturnal therapy allowing machine independence during the day for procedures or studies
19/20
Conclusions
✅Born to deliver a particular prescription with the available tools
✅Nomenclature & prescription has been motive for confusion
✅PIRRT & HYBRID are the terms that group ALL this therapies
✅We can group them in 2 types: CRRT-->iHD or iHD--> CRRT
Conclusions
✅Born to deliver a particular prescription with the available tools
✅Nomenclature & prescription has been motive for confusion
✅PIRRT & HYBRID are the terms that group ALL this therapies
✅We can group them in 2 types: CRRT-->iHD or iHD--> CRRT
20/20
Conclusions 2
✅Dosing should use equivalent clearances of other therapies
✅No evidence of better or worst outcomes than CRRT
✅Dosing & timing of medications is a MAYOR problem
✅Indications such as: night tx & transition to iHD are exlusive indications of PIRRT/HYBRID
Conclusions 2
✅Dosing should use equivalent clearances of other therapies
✅No evidence of better or worst outcomes than CRRT
✅Dosing & timing of medications is a MAYOR problem
✅Indications such as: night tx & transition to iHD are exlusive indications of PIRRT/HYBRID


















