
,
24 tweets,
7 min read
Read on Twitter
1/21 “Is there a nurse or doctor on board?”
Clinicians—have you ever responded to one of these?
Last week I left the hospital and boarded a flight for my vacation. I then responded to the mother of all in-flight emergencies…
Clinicians—have you ever responded to one of these?
Last week I left the hospital and boarded a flight for my vacation. I then responded to the mother of all in-flight emergencies…
2/ This was a flight with hundreds of people from Boston, so I estimated there would be at least 15 doctors. Turns out I was the only adult medicine doctor, BUT there was a cardiac nurse with me.
3/ The patient was middle-aged and experiencing crushing chest pain. We asked for the medical kit, took vital signs and performed an exam. By the way, you cannot hear sh*t through a stethoscope in the air. I could hear bilateral breath sounds, but that’s about it.
4/ The FAA mandates contents of medical kits for American airlines. I flew on a European airline, but the kit had most items & more. Of note: no pulse ox, no glucometer, few gloves, no Epi-pen, no Narcan. Some meds were in a different language without English translation. 

5/ We administered 325 mg aspirin and started the passenger on oxygen. You can deliver 2-4L oxygen by nasal cannula route. However, the tank will only last 1 hour or so.
6/ At this point I was very concerned the passenger was actually having an MI. The chest pain was ongoing, so we gave SL nitroglycerin, which significantly improved the chest pain and (fortunately) did not bottom out the blood pressure.
7/ In-flight medical emergencies are estimated to occur in 1/604 flights, or at an event rate of 24-130 per 1 million passengers. The most common type of emergency is syncope or near-syncope (32.7%) and cardiovascular symptoms account for only 7.0% of symptoms.

8/ I consulted with the ground medical doctor and pilot. I recommended diverting the plane. This is a complex decision that is ultimately made by the pilot in command. It only occurs in 4.4% of in-flight emergencies and costs $$$.
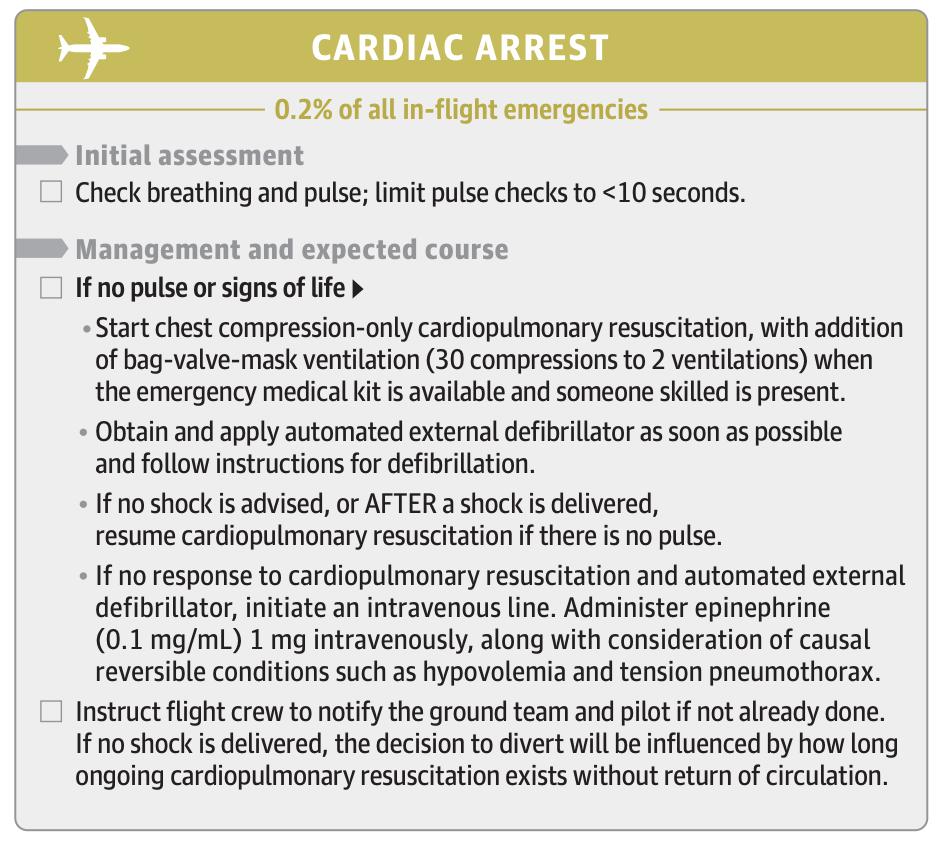
9/ Remember, even if you have just taken off, it takes at least 30 minutes to get from cruising altitude back to the ground…During descent I see that our passenger starts to slump forward in the seat. I get up and they are pulseless.
10/ I remove the passenger from the seat and the nurse promptly starts chest compressions. I ask for other passengers who are certified in CPR. I attached the AED pads to the chest and defibrillated ASAP. We give 2 more min of CPR and locate the Ambu-bag and epinephrine.
11/ BUT our passenger starts to move and talk! They are hypotensive and tachycardic. The nurse starts an IV and we start the 500cc bag of normal saline. We still have 20 minutes to go on descent. Fortunately, the vitals stabilize and there is not another arrest during landing.
12/ By the way, just try to picture landing sitting on the ground with your post-cardiac arrest patient surrounded by medical equipment and an entire cabin of people staring at you.
13/ The paramedics meet us on the tarmac and run a 12-lead ECG immediately. Well look what we have here…

14/ Our passenger makes it to the hospital!!
15/ Taking care of a cardiac arrest was one of the things I dreaded most about flying as a physician. It is exceedingly rare, accounting for only 0.3% of in-flight emergencies. Of in-flight events resulting in death, cardiac arrest accounts for 86% of cases.
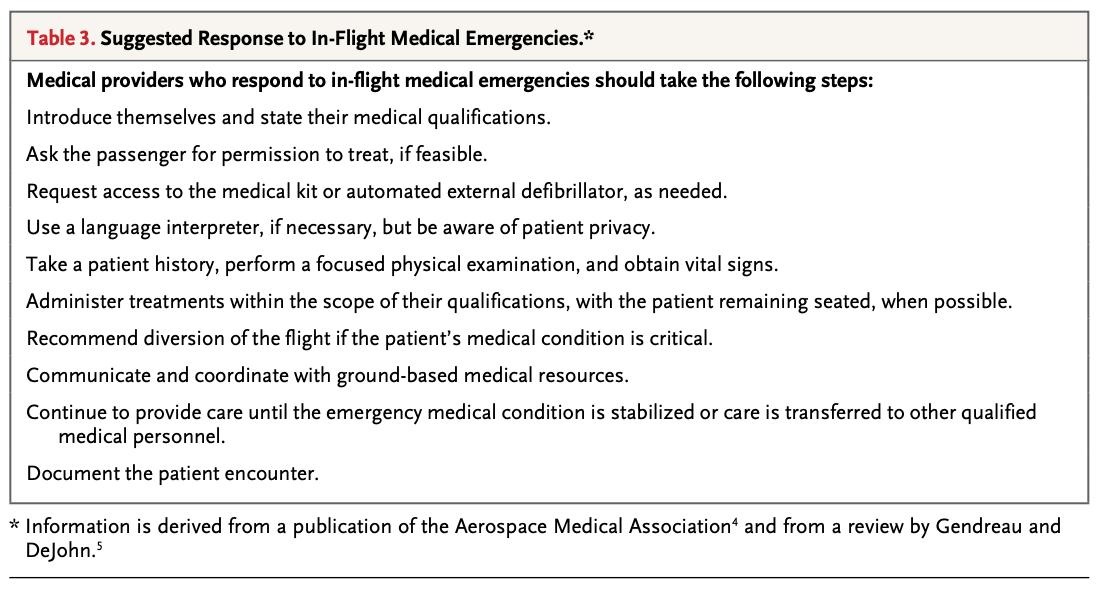
16/ A review by Martin-Gill et al. in JAMA 2018 (jamanetwork.com/journals/jama/…) includes short summaries of different medical emergencies and how you might respond as a clinician.
17/ In this case I felt most comfortable with the clinical medicine and least comfortable performing in a resource-limited setting with unfamiliar people, unclear rules, and high levels of pressure.
18/ This 2015 NEJM article provides a useful framework for approaching in-flight emergencies.
19/ Even though this circumstance had the best outcome possible, I wish some things could have been different. I wish we had established explicit team roles early.
20/ I wish I wore a watch on a regular basis (the nurse had one)! I wish a 3rd clinician had documented everything with explicit time stamps.
21/ I wish I could have had a full debrief with the flight crew and the nurse. I wish I could see the passenger and their family again.
Providing care in the air is a strange thing.
Providing care in the air is a strange thing.
Resources:
Martin-Gill. In-Flight Medical Emergencies: A Review: JAMA. 2018;320(24):2580-2590.
Peterson. Outcomes of Medical Emergencies on Commercial Airline Flights. NEJM 2013;368:2075-83.
Nable. In-Flight Medical Emergencies During Commercial Air Travel. NEJM 2015; 373:939-945
Martin-Gill. In-Flight Medical Emergencies: A Review: JAMA. 2018;320(24):2580-2590.
Peterson. Outcomes of Medical Emergencies on Commercial Airline Flights. NEJM 2013;368:2075-83.
Nable. In-Flight Medical Emergencies During Commercial Air Travel. NEJM 2015; 373:939-945
ECG-- from Life in the Fast Lane
asma.org/asma/media/AsM…
#tweetorial #airtravel #inflightemergency #physician #womeninmedicine #MedTwitter
*Details of this event were changed to protect the privacy of all involved.
asma.org/asma/media/AsM…
#tweetorial #airtravel #inflightemergency #physician #womeninmedicine #MedTwitter
*Details of this event were changed to protect the privacy of all involved.
Can’t believe how many people I’ve heard from who have been involved with in-flight medical emergencies. Also can’t believe how many paramedics and EMTs do this every day with no follow up and often in isolation. 👏















