
With Italy quarantining millions and contemplating critical care rationing in hospitals, and Iran's health system in chaos, it's fair to ask if this is possible in the US.
Bottom line is: the longer we wait to act, the more likely it becomes.
I've made some charts.
Bottom line is: the longer we wait to act, the more likely it becomes.
I've made some charts.
This builds on @ScottGottliebMD's excellent 🧵laying out where we're headed and what to do about it.
Bear in mind while reading this that the US has already lost 6-7 weeks of potential domestic preparedness - due to the testing debacle and emphasis on overseas risks rather than domestic spread (as my @nytopinion piece lays out). nytimes.com/2020/03/07/opi…
Biggest risk in coming weeks: US cities produce so many critical cases that hospitals are overwhelmed. This creates a doom loop in which care quality suffers and mortality spikes.
That's likely why mortality was so much higher in Wuhan than rest of China. (From WHO rpt👇)
That's likely why mortality was so much higher in Wuhan than rest of China. (From WHO rpt👇)

Let's get oriented.
These three curves show diff rates of new weekly critical cases over time, assuming action starts at point (0).
Critical cases appear to be roughly 5% of total, and need intensive care to survive.
These three curves show diff rates of new weekly critical cases over time, assuming action starts at point (0).
Critical cases appear to be roughly 5% of total, and need intensive care to survive.
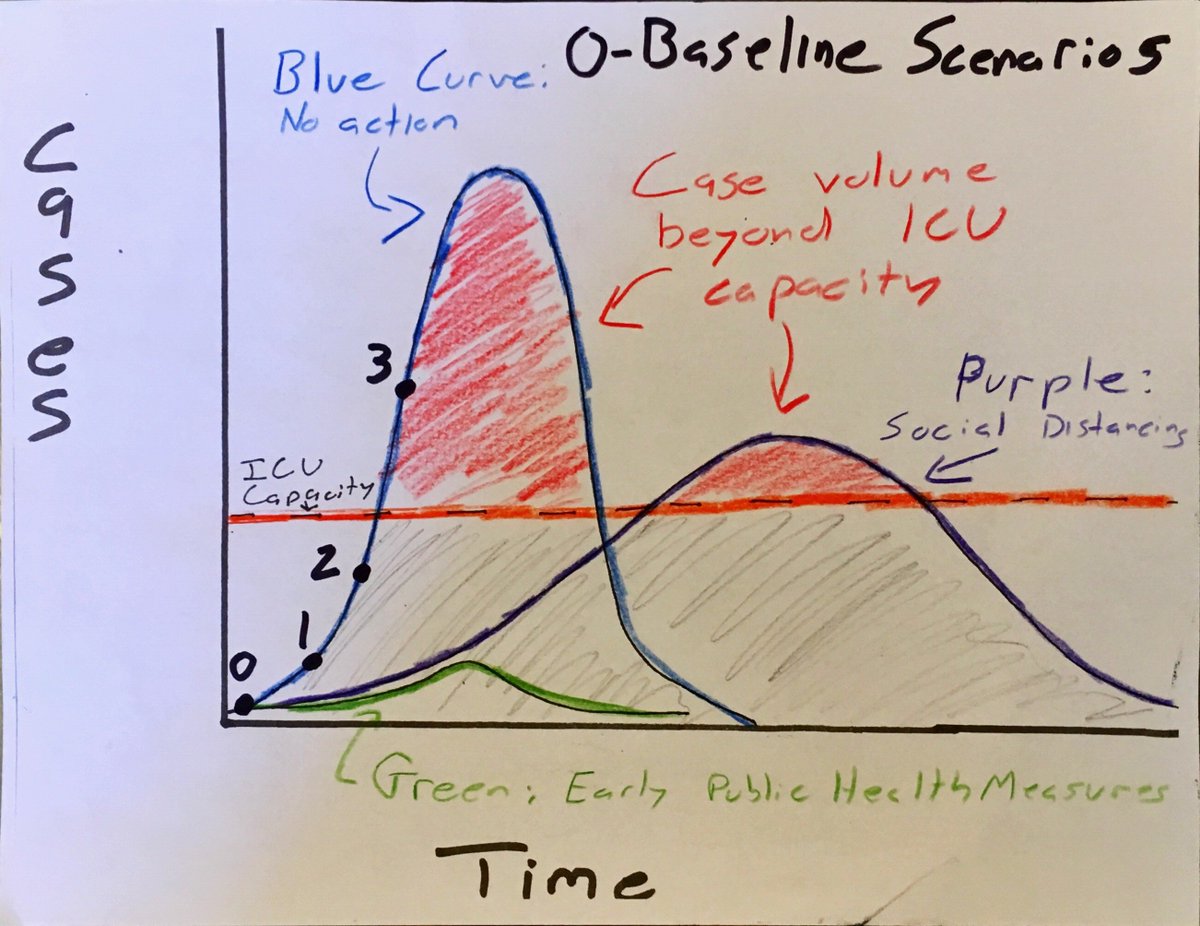
(Caveat - the charts are *indicative*. Intended to conceptually convey cost of delaying action. NOT drawn to perfect scale, etc.)
So, blue curve: no action taken. Exponential growth until virus starts to run low on new hosts (b/c so many already recovered/immune, or dead).
So, blue curve: no action taken. Exponential growth until virus starts to run low on new hosts (b/c so many already recovered/immune, or dead).

Purple Curve: Social distancing measures applied starting from point (0). Same number of total cases (volume under curve) but much lower peak, longer duration.

Green Curve: early, robust public health measures applied from (0) (contact tracing, targeted household quarantine, etc). When applied before cases have widely spread, these can lock down or greatly limit an outbreak. But become harder to scale up as case numbers grow.

Orange line represents baseline absorptive capacity in ICUs.
The red shading above ICU line represents new cases emerging beyond capacity. This is the greatest mortality risk.
The red shading above ICU line represents new cases emerging beyond capacity. This is the greatest mortality risk.
Hopkins paper estimates ~46,500 ICU beds in the US, with theoretical potential to double that with enough advance notice.
And a 2015 paper estimates that ICU occupancy rates are on average around ~66%.
centerforhealthsecurity.org/cbn/2020/cbnre…
ncbi.nlm.nih.gov/pmc/articles/P…
And a 2015 paper estimates that ICU occupancy rates are on average around ~66%.
centerforhealthsecurity.org/cbn/2020/cbnre…
ncbi.nlm.nih.gov/pmc/articles/P…


Occupancy rates are probably higher now, due to flu season.
But for our purposes here, the takeaway is that ICU beds are limited and quite occupied already, but have some potential to stretch if given enough advance notice to expand capacity.
But for our purposes here, the takeaway is that ICU beds are limited and quite occupied already, but have some potential to stretch if given enough advance notice to expand capacity.
Of course, you don't trigger action at point (0).
You trigger once virus' risk profile is understood, *and* this translates into political will for decisive action.
So these scenarios explore 3 points at which that may occur, and how timing of choice affects health outcomes.
You trigger once virus' risk profile is understood, *and* this translates into political will for decisive action.
So these scenarios explore 3 points at which that may occur, and how timing of choice affects health outcomes.
Scenario (1): early decisive action. Public health measures (green) & social distancing measures (purple) triggered at point (1), while cases are still low.
Volume of cases is only the gray shaded area; much less than either social distancing or inaction.
Volume of cases is only the gray shaded area; much less than either social distancing or inaction.

Call this roughly the Singapore approach.
Limits both case numbers and duration, and keeps cases below ICU capacity.
This minimizes overall mortality, and overall social disruption. Measures are still disruptive, but not as extreme as next scenarios.
Limits both case numbers and duration, and keeps cases below ICU capacity.
This minimizes overall mortality, and overall social disruption. Measures are still disruptive, but not as extreme as next scenarios.
(2) Delayed action scenario.
Measures applied at point (2), only once cases growth has accelerated, but still somewhat before hospitals are overwhelmed and mortality begins to spike.
Delayed action can mitigate over-saturation of hospitals but not avert it.
Measures applied at point (2), only once cases growth has accelerated, but still somewhat before hospitals are overwhelmed and mortality begins to spike.
Delayed action can mitigate over-saturation of hospitals but not avert it.
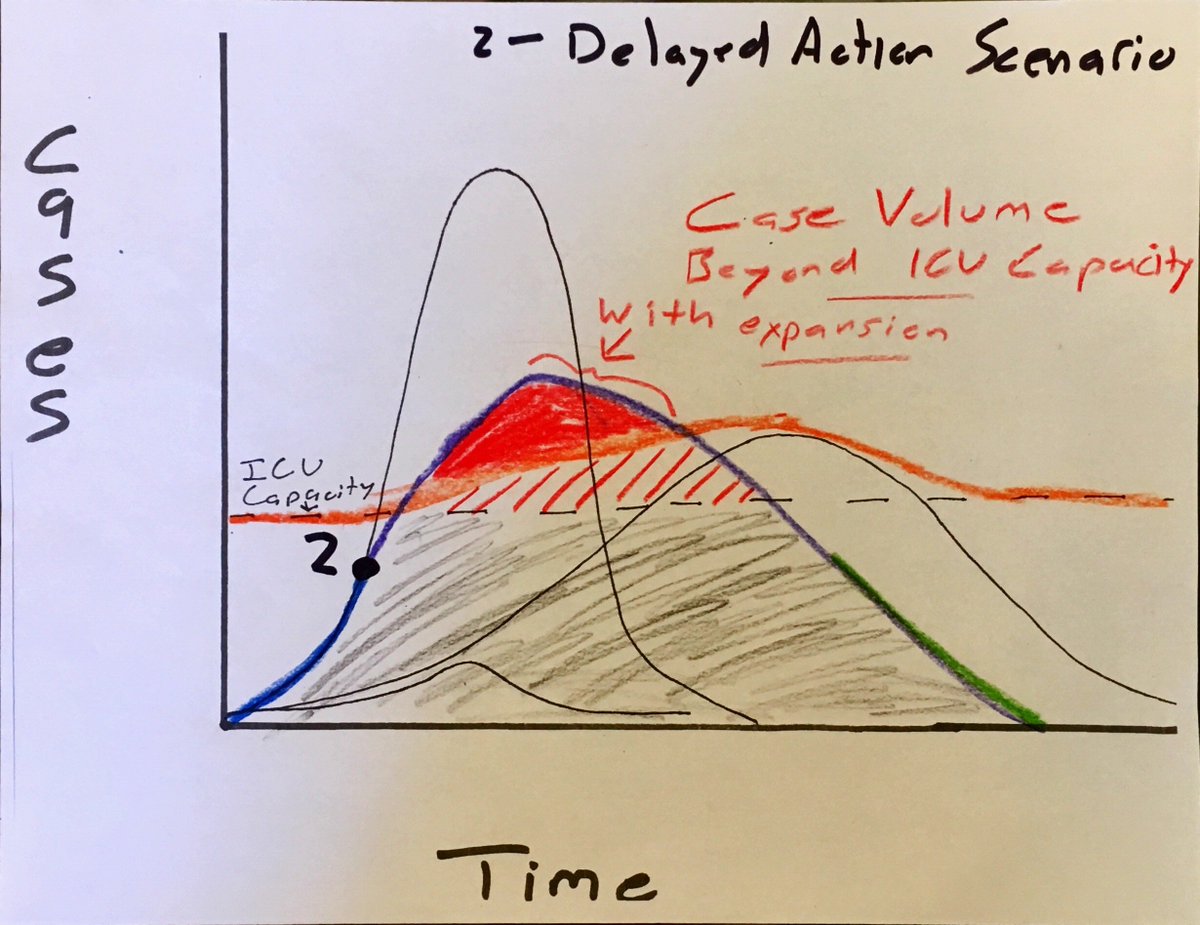
In this scenario, social distancing measures are triggered late, and case volumes are too high for contact tracing to meaningfully reach many/most cases.
Measure to stretch ICU capacity are triggered at (2) and slowly add capacity, eventually catching up to excess cases.
Measure to stretch ICU capacity are triggered at (2) and slowly add capacity, eventually catching up to excess cases.

Even with stretching of ICU capacity, substantial volume of excess critical cases (dark red). But red stripes show volume of additional cases that could be managed if capacity is expanded. Capacity catches up to cases earlier.
This is a version of China's approach.
This is a version of China's approach.

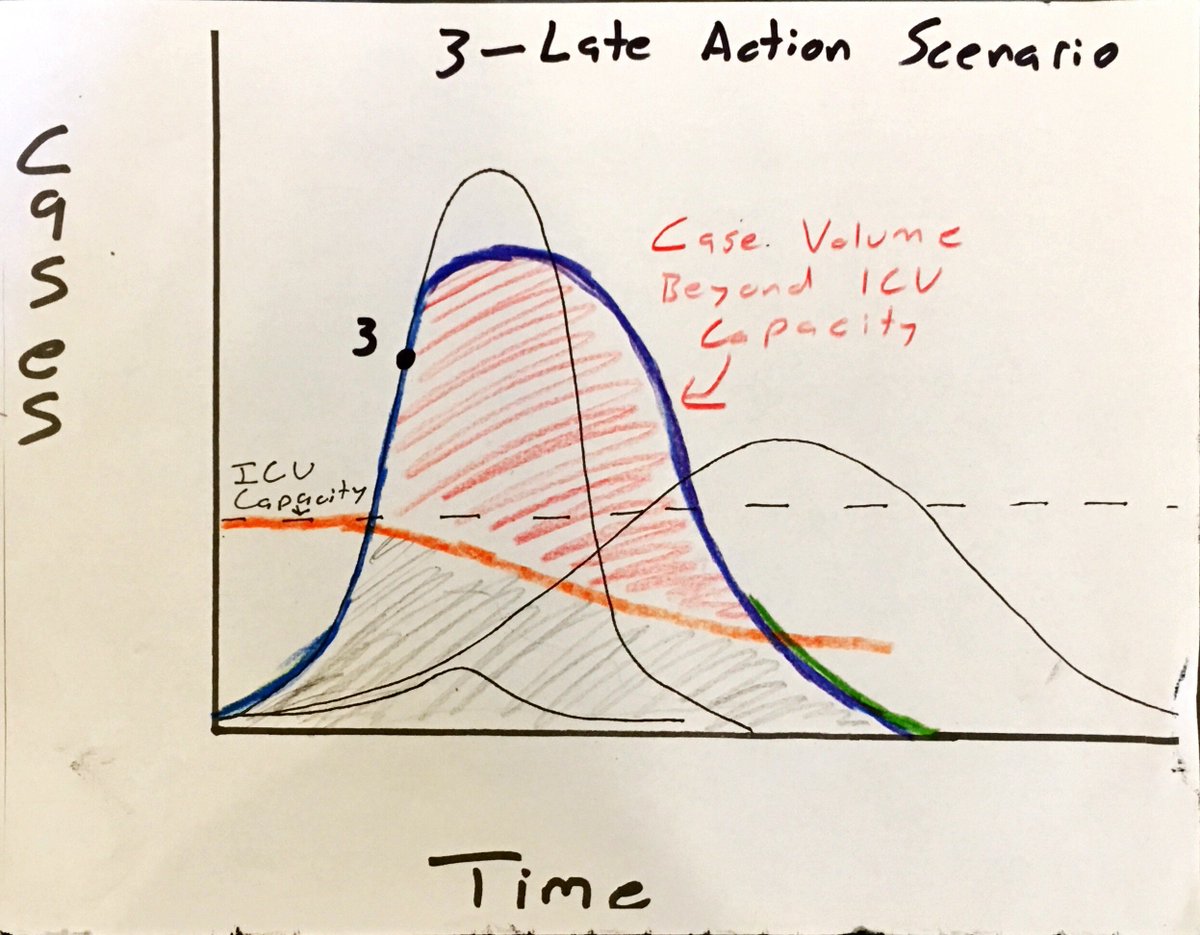
Scenario (3): the doom loop.
Action taken very late, once critical cases are already overwhelming hospital capacity.
These circumstances can actually *degrade* ICU absorptive capacity, because facilities become overwhelmed, standards suffer, staff start getting infected.
Action taken very late, once critical cases are already overwhelming hospital capacity.
These circumstances can actually *degrade* ICU absorptive capacity, because facilities become overwhelmed, standards suffer, staff start getting infected.

If action isn't triggered until point (3), case volume is so extreme that public health measures are mostly out the window and social distancing measures have less impact. And hospitals are already beginning to lose staff to illness, meaning less ability to stretch ICU capacity.
This means an extremely high volume of critical cases paired with declining hospital capacity to treat them. This creates a mortality rate doom loop. Iran may be facing this sort of scenario.
And getting this back on track requires the most disruptive measures of any scenario.
And getting this back on track requires the most disruptive measures of any scenario.
(NB - just realized the purple curve as drawn seems to indicate (3) has a comparable/higher volume of cases than inaction. That's just my poor artistry; total case volume in (3) would be somewhat lower but perhaps not dramatically so)
So the takeaway here: TIMING MATTERS IMMENSELY.
Triggering readiness measures before they appear urgently necessary (Scen 1) can keep things under control.
Triggering readiness measures before they appear urgently necessary (Scen 1) can keep things under control.

Triggering dramatic measures once they're obviously *going to be needed* (2) can help, but still leaves a pretty desperate phase.

Waiting to trigger measures until people are being turned away from hospitals (3) is a cataclysm.
And this is why public health folks in your twitter feed are freaking out, and why the US testing debacle is so extraordinarily damaging.
We lost 6-7 weeks of potentially triggering earlier action, because lack of testing made us blind.
We lost 6-7 weeks of potentially triggering earlier action, because lack of testing made us blind.
And the continuing testing gaps in the US means we still don't know which US cities could be nearing point 1, point 2, or point 3 on the curve.
That's hugely important because extremity of actions must be calibrated accordingly.
So we're still losing time, even today.
/end
That's hugely important because extremity of actions must be calibrated accordingly.
So we're still losing time, even today.
/end








