,
76 tweets,
19 min read
Read on Twitter
Heh heh, the Amazing Yuripridio, world-conquering hypnotist 

But we must be careful on this. I have a PhD student at #ORBITA hq called Frances Wood. I met her first as a manager in a research unit a few years ago. She was the nicest, kindest person there, who would always make me tea when I visited anyone in the unit.
By and by, she wrote a PhD proposal with me. She was a trained nurse, as many of that unit's staff are. But when we submitted the grant, I discovered in her CV that she was also secretly a trained psychologist.
So while I have @DrJHoward @mshunshin et al leaping out to attack me, Cato-like [security cam footage: youtube.com/embed/FbUD7FRS…] on any mathematical, statistical, and programming inexactitudes, I also have Frances patiently explaining the finer points of psychology to me.
She patiently teaches me the following:
Q C30.
The Amazing Yuripridio wants me to think my statin is making me sleepy.
Which of these can he do?
(A) *Make me sleepy* by suggestion after I take my statin.
(B) Wait for me to be sleepy, and then point out I'm on a statin.
Q C30.
The Amazing Yuripridio wants me to think my statin is making me sleepy.
Which of these can he do?
(A) *Make me sleepy* by suggestion after I take my statin.
(B) Wait for me to be sleepy, and then point out I'm on a statin.
Let's look at some of the questions/comments so far.
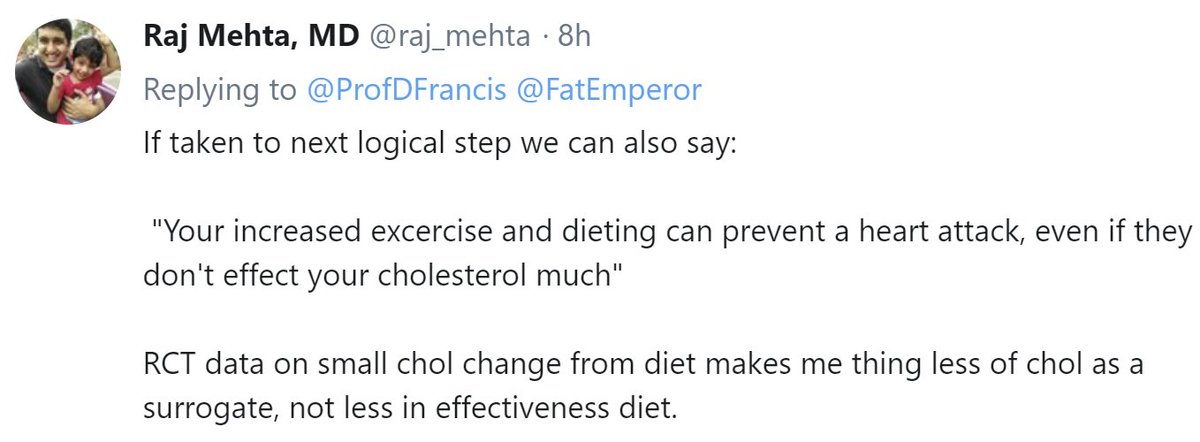
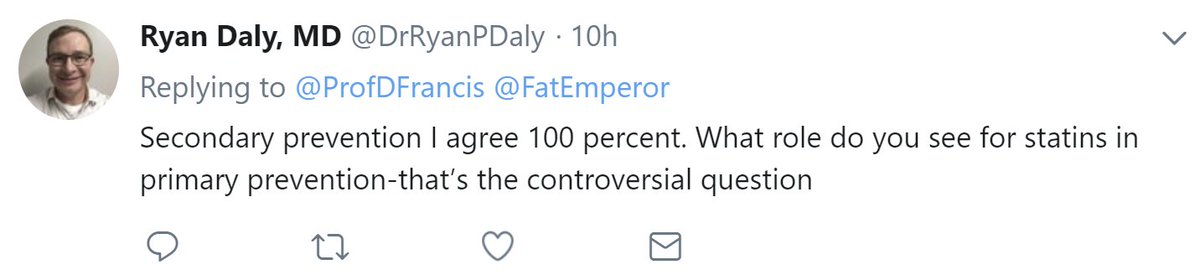
Raj Mehta points out that there is much more benefit diet and exercise than merely cholesterol reduction.
Raj Mehta points out that there is much more benefit diet and exercise than merely cholesterol reduction.
[Thanks for the SMSs that there were 2 C30's. I have decided to say that was for "security reasons", which is what I always say when I make an inexplicable mistake.]
Q C31
Since I genuinely believe in diet & exercise, why don't I tell patients to use them *to lower cholesterol*?
Q C31
Since I genuinely believe in diet & exercise, why don't I tell patients to use them *to lower cholesterol*?
brings up an important question
All my above rambling was about primary prevention, i.e. for people who appear perfectly healthy: never had angina or a heart attack
Secondary prevention seems different. But is it a different disease, or the same with higher stakes?
All my above rambling was about primary prevention, i.e. for people who appear perfectly healthy: never had angina or a heart attack
Secondary prevention seems different. But is it a different disease, or the same with higher stakes?
Question C32
Imagine you are a bit of plaque in some dude, waiting to chip off, expose the plaque interior to platelets and cause an MI.
Do you have any way to find out if any of your colleague bits of plaque have *ever* done the same, in the patient's lifetime so far?
Imagine you are a bit of plaque in some dude, waiting to chip off, expose the plaque interior to platelets and cause an MI.
Do you have any way to find out if any of your colleague bits of plaque have *ever* done the same, in the patient's lifetime so far?
Question C33.
Olly is a plaque in a patient with a previous MI.
Paul is a plaque in a patient with no previous MI (but similar amount of atheroma)
Roughly speaking, how will Olly and Paul respond to (say) statins?
Let's suppose we don't know how statins work (I certainly don't)
Olly is a plaque in a patient with a previous MI.
Paul is a plaque in a patient with no previous MI (but similar amount of atheroma)
Roughly speaking, how will Olly and Paul respond to (say) statins?
Let's suppose we don't know how statins work (I certainly don't)
Question C34.
Reminder:
Olly is in person with Old MI
Paul is in person without
Taking about 1000 Ollies, and 1000 Pauls, in patients with similar atheroma quantities, given the history of events, which are more likely to have an event in years to come?
(Assume NO treatment)
Reminder:
Olly is in person with Old MI
Paul is in person without
Taking about 1000 Ollies, and 1000 Pauls, in patients with similar atheroma quantities, given the history of events, which are more likely to have an event in years to come?
(Assume NO treatment)
*ONLY READ AFTER TRYING THE ABOVE*
Plaques can't talk to each other reliably, and even if they could they can never tell if the patient has (or had!) *symptomatic* angina.
They are therefore *unable* to respond differently in primary and secondary situations.
Plaques can't talk to each other reliably, and even if they could they can never tell if the patient has (or had!) *symptomatic* angina.
They are therefore *unable* to respond differently in primary and secondary situations.
All they can do is just be more risky in the (untreated) secondary situation [Ollies], because for numerous complex reasons the Ollies are from a body whose genes, diet, exercise and life experience have led to a rupture in the past.
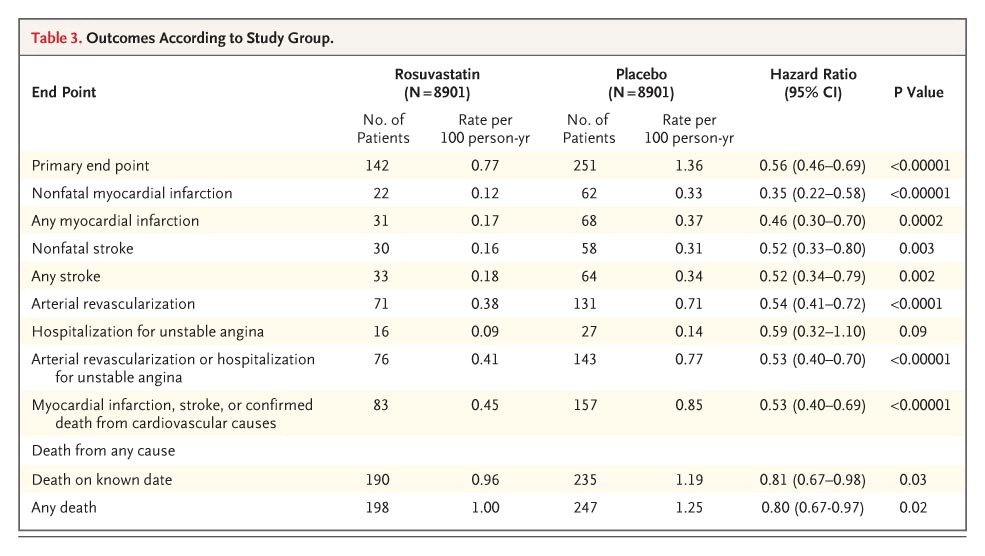
Here's table 3 from:
ndph.ox.ac.uk/files/forms/eu…
Here's table 3 from:
ndph.ox.ac.uk/files/forms/eu…
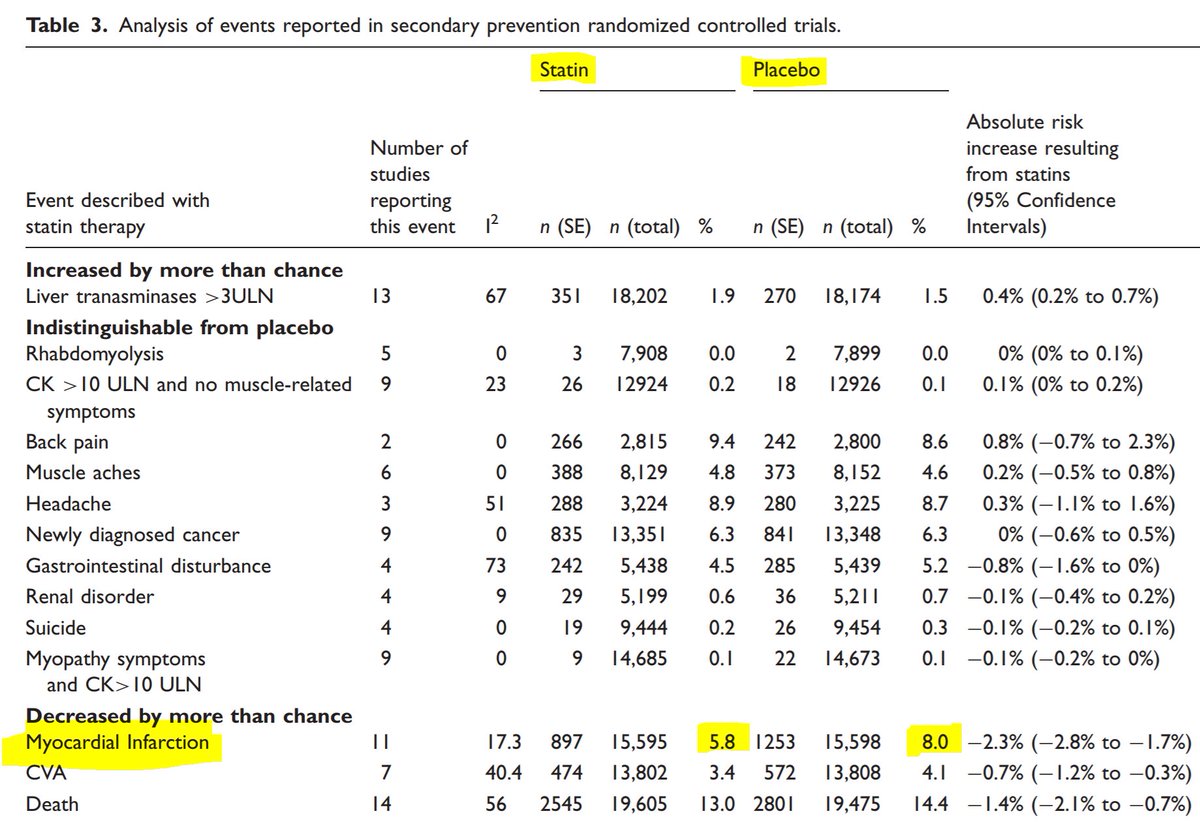
Question C35.
In Judy Finegold's above meta-analysis table of SECONDARY prevention by statin-versus-placebo, roughly what proportion of MI's are prevented by statins?
(This is asking about RELATIVE risk reduction; we will discuss absolute later)
In Judy Finegold's above meta-analysis table of SECONDARY prevention by statin-versus-placebo, roughly what proportion of MI's are prevented by statins?
(This is asking about RELATIVE risk reduction; we will discuss absolute later)
Here is the PRIMARY prevention table from her same paper.
Again please find the RELATIVE risk reduction of MI's.
That is to say, of the MI's that would have happened on placebo, what percentage were prevented in the statin arm?
Again please find the RELATIVE risk reduction of MI's.
That is to say, of the MI's that would have happened on placebo, what percentage were prevented in the statin arm?
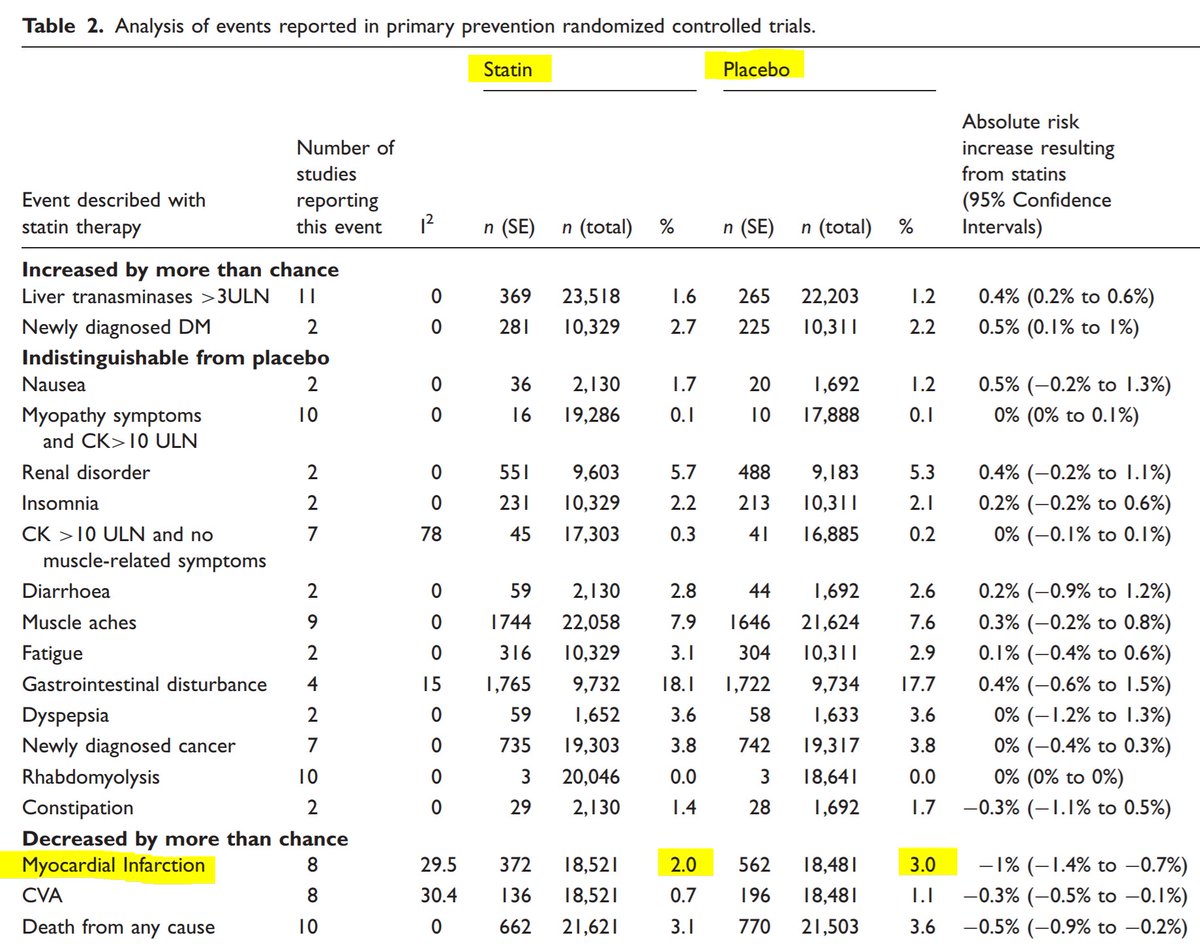
Question C36.
In the above PRIMARY prevention table, the relative risk reduction for MI, by statins, is:
In the above PRIMARY prevention table, the relative risk reduction for MI, by statins, is:
Think about whether these RELATIVE risk reductions are similar between the two patient groups: those before a first event and those after? Or are they wildly different?
The amazing YuriPridio turns out to be a doctor as well as a hypnotist. He has tweeted this:
The amazing YuriPridio turns out to be a doctor as well as a hypnotist. He has tweeted this:
80,000 patients have done placebo-controlled trials of statin
6,000 died during the trials
They have sent you a message which you have calculated by your own hand.
No tricks.
Q C37.
Are statins equally effective (in RRR terms) in primary versus secondary prevention?
6,000 died during the trials
They have sent you a message which you have calculated by your own hand.
No tricks.
Q C37.
Are statins equally effective (in RRR terms) in primary versus secondary prevention?
raised the question of absolute versus relative risks.
This is important, because even a 99% relative risk reduction of something that never happen (e.g. abduction by aliens) isn't exciting.
But look at this pdfs.semanticscholar.org/bc5b/62c4da447…
This is important, because even a 99% relative risk reduction of something that never happen (e.g. abduction by aliens) isn't exciting.
But look at this pdfs.semanticscholar.org/bc5b/62c4da447…
May I pause here to point out a problem we have as a community? We have many more answers to C37 than to C35 and C36, which C37 explicitly relies on.
At 7 votes, the *majority of answers* to C37 are wrong. I wonder if this is because people aren't doing the arithmetic?
At 7 votes, the *majority of answers* to C37 are wrong. I wonder if this is because people aren't doing the arithmetic?
This thread (and me in general) is only for people who want to work things out for themselves
If people don't like thinking
or using numbers
or developing a mastery of their field,
don't ask me what to do
There are others who will tell you what to do
Obey a guideline, not me😀
If people don't like thinking
or using numbers
or developing a mastery of their field,
don't ask me what to do
There are others who will tell you what to do
Obey a guideline, not me😀
But just a few seconds of that video will wash away any tricky questions from patients.
No side branches to wreck
No requirement to dissect intima
Cholesterol melts away on demand
Artery beautifully smooth and healthy after
Hell, *I* would take that PCI over any I really do 🤣
No side branches to wreck
No requirement to dissect intima
Cholesterol melts away on demand
Artery beautifully smooth and healthy after
Hell, *I* would take that PCI over any I really do 🤣
Another A Garg special. If you pay per stent, what do you get?
Sorry got distracted there. Back to the question of why we need to think about RRR sometimes, ARR sometimes, and *neither* sometimes.
If we aren't fluent in the numbers, we are at the whim of any charlatan or rabble rouser.
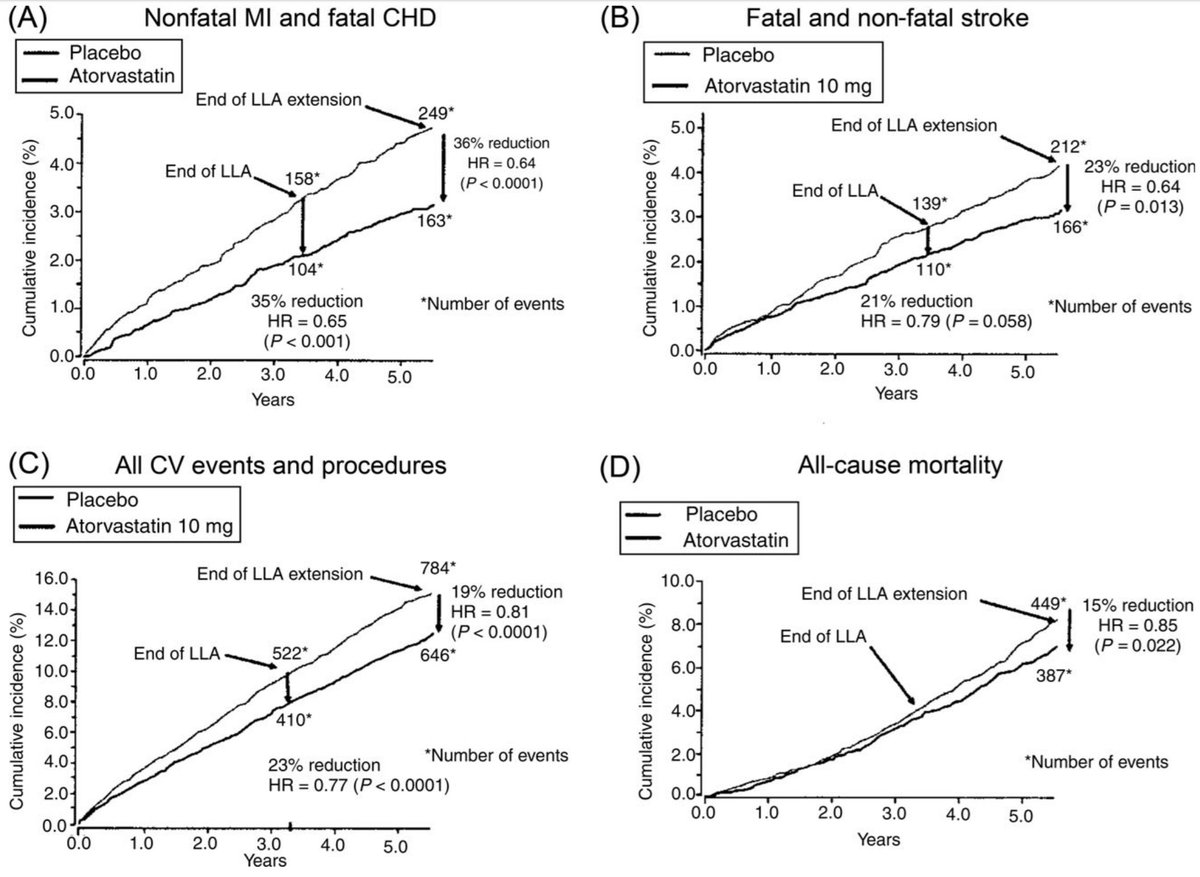
Here's the pic again.
If we aren't fluent in the numbers, we are at the whim of any charlatan or rabble rouser.
Here's the pic again.
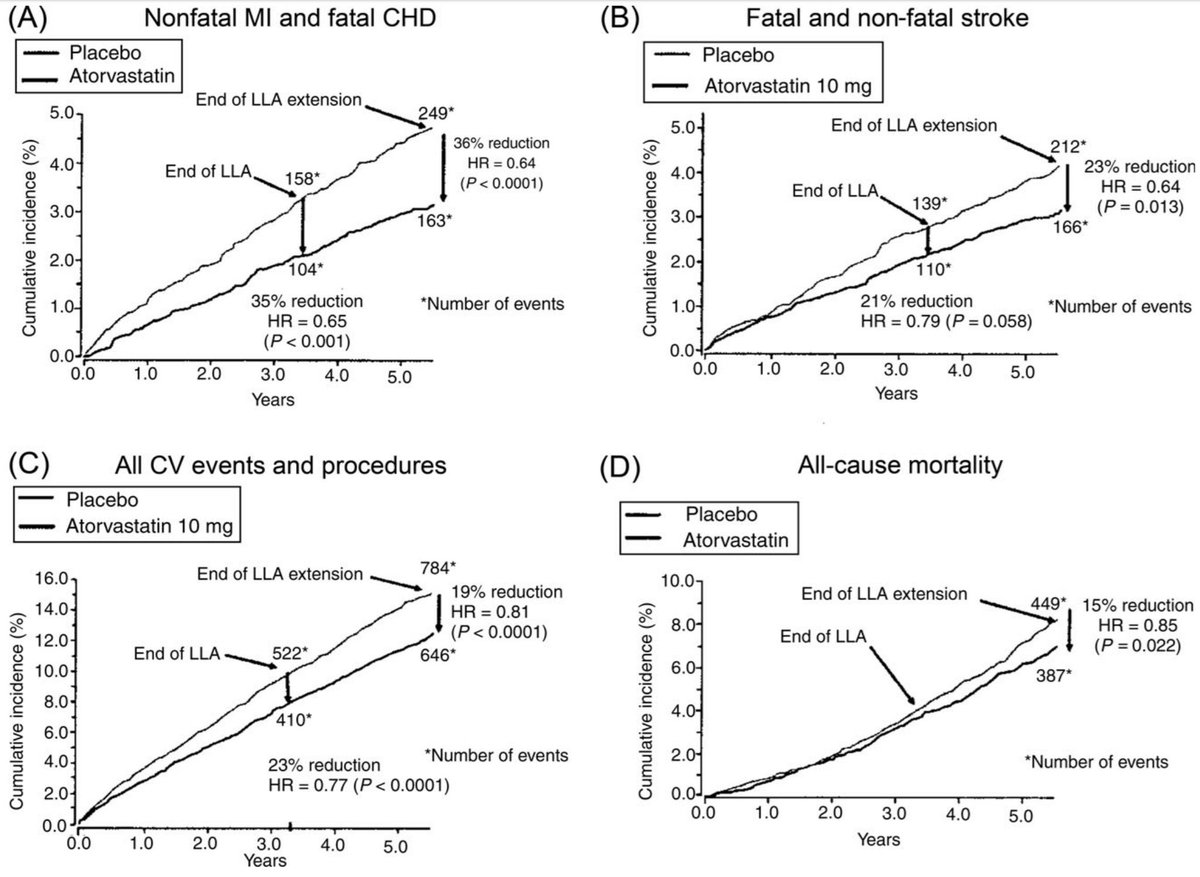
C38
Focus on Panel A (top left).
What is the ABSOLUTE risk reduction (vertical distance between the curves):
(a) at 1.0 years?
(b) at 3 and a bit years?
(c) at 5 and a bit years?
Just guess it by eye.
Focus on Panel A (top left).
What is the ABSOLUTE risk reduction (vertical distance between the curves):
(a) at 1.0 years?
(b) at 3 and a bit years?
(c) at 5 and a bit years?
Just guess it by eye.
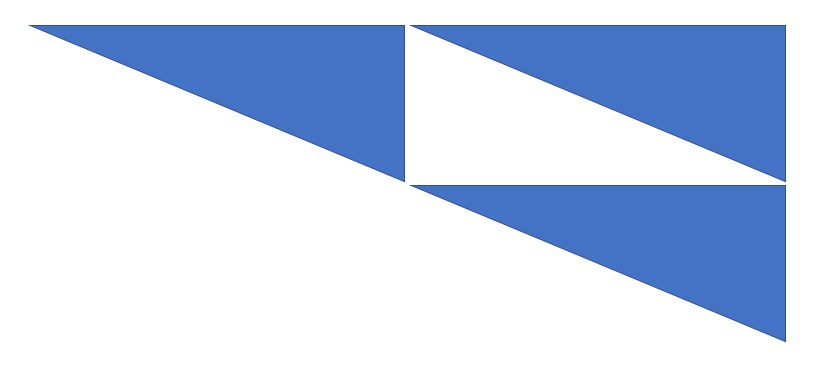
Look at this image from junior school math at magoosh.com/hs/uncategoriz…
What is it trying to illustrate?
Can you remember what these three triangles are called?
Equilateral?
Congruent?
Similar?
Isoceles?
Reflex?
Scalene?
What is it trying to illustrate?
Can you remember what these three triangles are called?
Equilateral?
Congruent?
Similar?
Isoceles?
Reflex?
Scalene?
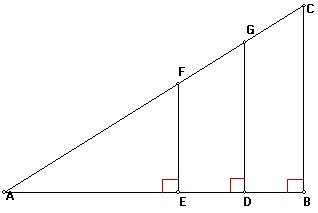
C39
Even if you can't quite remember the name, what do you *know* about these ratios:
FE/AE
GD/AD
CB/AB
Even if you can't quite remember the name, what do you *know* about these ratios:
FE/AE
GD/AD
CB/AB
C40.
Compare the math book triangle above, with the survival curve.
Obviously they are left-right swapped.
But the triangle I want you to focus on is that BETWEEN the survival curves (not the x axis).
The height of the triangle (absolute risk reduction)
Compare the math book triangle above, with the survival curve.
Obviously they are left-right swapped.
But the triangle I want you to focus on is that BETWEEN the survival curves (not the x axis).
The height of the triangle (absolute risk reduction)
C41. So which is the correct absolute risk reduction to quote?
C42.
When describing AVERAGE effects of lifelong therapies in populations, why do prevention scientists not always talk about absolute risk reduction?
When describing AVERAGE effects of lifelong therapies in populations, why do prevention scientists not always talk about absolute risk reduction?
First vote is for conspiracy. I sympathise 8-) but don't agree.
I explain RRR to patients like this.
"Think of all the people you know who have had a heart attack. If they had all taken a statin instead of not, one third *of them* would not have had that heart attack."
I explain RRR to patients like this.
"Think of all the people you know who have had a heart attack. If they had all taken a statin instead of not, one third *of them* would not have had that heart attack."
That leverages human experience, and allows patients to judge more naturally what they want to do.
We all make judgements based on contingent probabilities: shall I take an umbrella?
Based on how likely it is to rain, and how much better off I will be with one *IF* it rains.
We all make judgements based on contingent probabilities: shall I take an umbrella?
Based on how likely it is to rain, and how much better off I will be with one *IF* it rains.
C43.
Quentin and Robert are brothers with identical risk factors, except Quentin is 10 years older.
Have a look at this graph from a free-to-read Judy Finegold paper ncbi.nlm.nih.gov/pubmed/23218570
Quentin and Robert are brothers with identical risk factors, except Quentin is 10 years older.
Have a look at this graph from a free-to-read Judy Finegold paper ncbi.nlm.nih.gov/pubmed/23218570
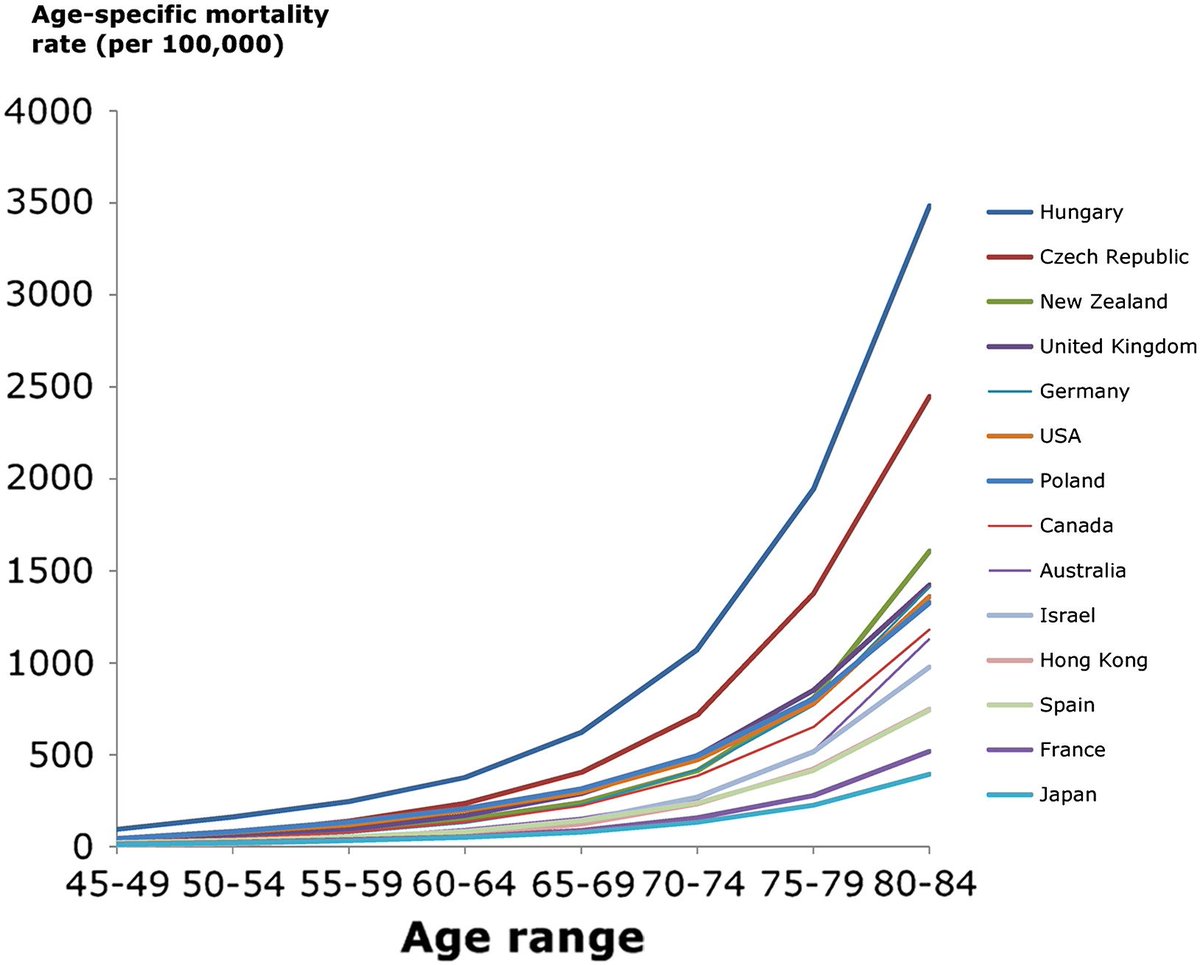
C43.
By what proportion is Quentin's CV risk greater than Robert's?
I haven't told you what country they are from.
If you think it matters, suppose it is Hungary (easiest to calc)
By what proportion is Quentin's CV risk greater than Robert's?
I haven't told you what country they are from.
If you think it matters, suppose it is Hungary (easiest to calc)
Q44.
Robert has a younger brother, Steven, who arrives late to the sermon.
Which value, as an effect size of statins, will be the same for him?
Robert has a younger brother, Steven, who arrives late to the sermon.
Which value, as an effect size of statins, will be the same for him?
Q45.
Oh! Out of Robert's pocket falls a half-empty packet of cigarettes. He looks sheepish.
Which value, as an effect size of statins, will *still in light of this* be the same for him?
Oh! Out of Robert's pocket falls a half-empty packet of cigarettes. He looks sheepish.
Which value, as an effect size of statins, will *still in light of this* be the same for him?
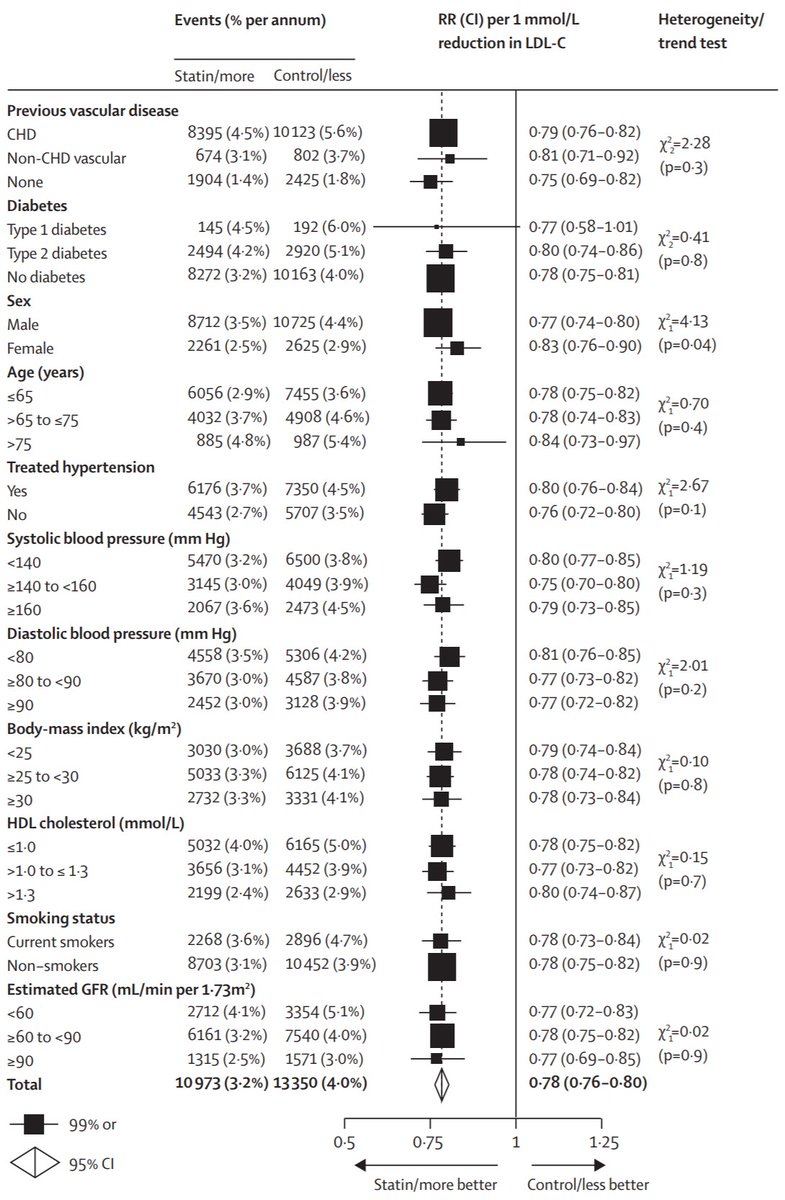
Now it is time to read one of the most important prevention analyses of all time. The CTT 2010
thelancet.com/pdfs/journals/…
And its Figure 3, the most important, most time-saving, most stress-relieving figure of all time for prevention docs and their patients.
Gaze and marvel!
thelancet.com/pdfs/journals/…
And its Figure 3, the most important, most time-saving, most stress-relieving figure of all time for prevention docs and their patients.
Gaze and marvel!
I know about a quarter of the people who put this together. There never was a more widely disparate group of characters, each ingenious in their own way, and each ambitious to be first out with the truth. It's a miracle they worked together on this.
If there was a conspiracy, one of them would *definitely* blow the whistle, if only to lord it over the others.
Their mutual distrust and habitual manoeuvering is what makes me confident there is nothing wrong with their data
They're like the Game of Thrones
Less nudity though
Their mutual distrust and habitual manoeuvering is what makes me confident there is nothing wrong with their data
They're like the Game of Thrones
Less nudity though
C46.
The graph above, Fig 3 of CTT 2010, shows *relative* risk reduction in subgroups of the thousands of randomized patients.
Remember Steve has just been outed to be a smoker?
On the graph, what is the difference between the effectiveness in smokers versus nonsmokers?
The graph above, Fig 3 of CTT 2010, shows *relative* risk reduction in subgroups of the thousands of randomized patients.
Remember Steve has just been outed to be a smoker?
On the graph, what is the difference between the effectiveness in smokers versus nonsmokers?
If you work through the reasoning above, hopefully you will accept that at a *scientific* level, the RELATIVE risk is the most helpful (i.e. least individual-dependent) way to discuss and compare effects of preventative steps *for a group*.
thanks for your patience
I have to tell everyone I get very annoyed at some of the things Aseem writes. Then I meet him at a debate and he is so handsome and generous and kind that I end up hugging him and finding common ground
Infuriating for an old git like me
I have to tell everyone I get very annoyed at some of the things Aseem writes. Then I meet him at a debate and he is so handsome and generous and kind that I end up hugging him and finding common ground
Infuriating for an old git like me
My friend Aseem seems to have fallen into the trap laid at thennt.com/nnt/statins-pe… (the link in his tweet).
My fellow Cardiology TPD Dr Becky Lane, and I, trained Aseem, and I think I signed his CCT in Cardiology, so I am biased against criticising his logic.
And he is handsome
My fellow Cardiology TPD Dr Becky Lane, and I, trained Aseem, and I think I signed his CCT in Cardiology, so I am biased against criticising his logic.
And he is handsome
The above page focusses on patients at low risk.
CTT 2010 Figure 3 is again key here so please excuse me for re-plagiarising it.
CTT 2010 Figure 3 is again key here so please excuse me for re-plagiarising it.
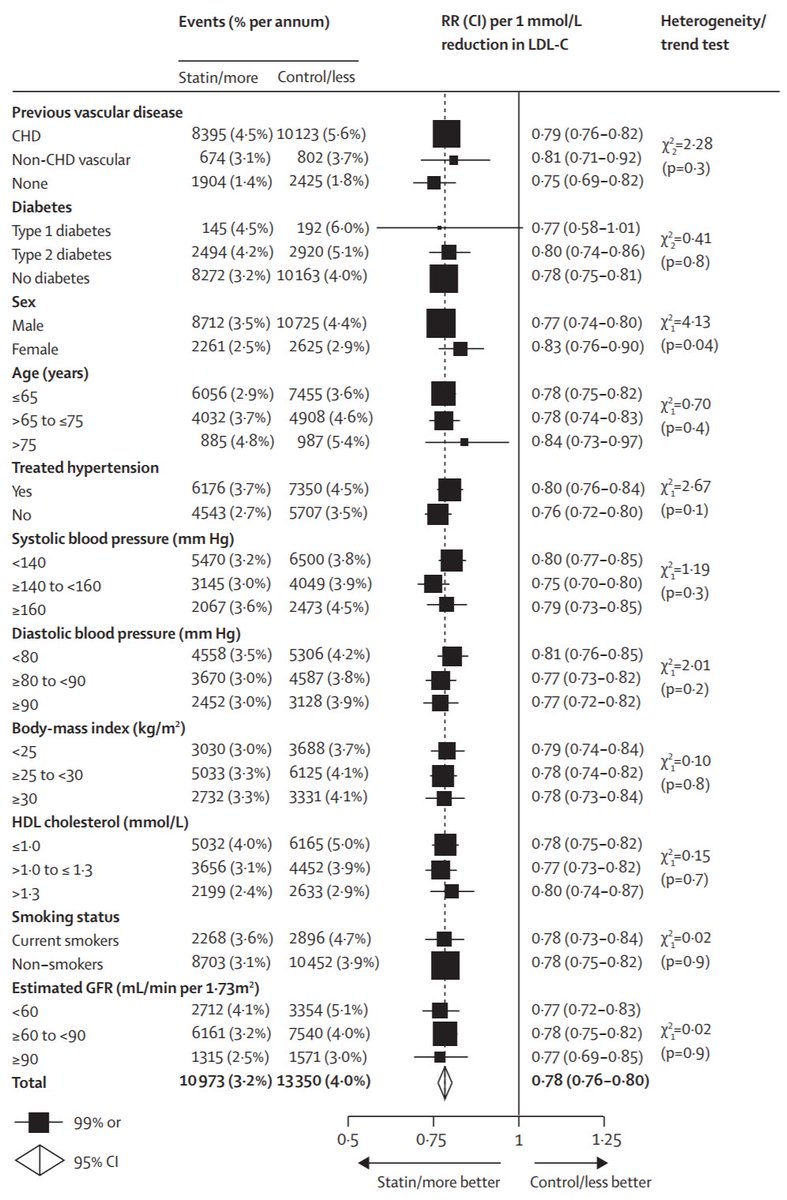
C47.
Which of these low-risk subgroups see a *significantly* (i.e. interaction P value <0.05, in last column) weaker Relative Risk Reduction from statins
Which of these low-risk subgroups see a *significantly* (i.e. interaction P value <0.05, in last column) weaker Relative Risk Reduction from statins
C48.
(a) In the group you chose, what is the relative risk reduction?
(b) In the rest of the patients (i.e. those who don't have that low-risk feature) what is the Relative Risk Reduction?
Just give your best estimates (the point estimate or central value)
It's per mM LDL redn
(a) In the group you chose, what is the relative risk reduction?
(b) In the rest of the patients (i.e. those who don't have that low-risk feature) what is the Relative Risk Reduction?
Just give your best estimates (the point estimate or central value)
It's per mM LDL redn
Cant tell if people are trolling or just finding it tricky
First 2 ans to C47 different, both wrong
Try this. Look down the right hand column, of p values. They are for heterogeneity, i.e. indicate if subgroups seem more different than usually occurs by chance
Where is p<0.05?
First 2 ans to C47 different, both wrong
Try this. Look down the right hand column, of p values. They are for heterogeneity, i.e. indicate if subgroups seem more different than usually occurs by chance
Where is p<0.05?
OK, reality coming into the lead again.
Given what *you* have deduced from the data, RRR is the most consistent feature of statin effect across groups.
RRR almost invariant across all subgroups. A bit weaker in women (although many subgroup tests, so could be fluke #bonferroni)
Given what *you* have deduced from the data, RRR is the most consistent feature of statin effect across groups.
RRR almost invariant across all subgroups. A bit weaker in women (although many subgroup tests, so could be fluke #bonferroni)
C49.
Therefore in even lower risk patients those typical of CTT 2010, e.g. younger etc. what do you *GUESS* will be the relative risk reduction?
Therefore in even lower risk patients those typical of CTT 2010, e.g. younger etc. what do you *GUESS* will be the relative risk reduction?
And here is the plot from Paul Ridker's JUPITER trial. nejm.org/doi/pdf/10.105…
It shows heart attack/stroke/death from cardiac causes.
What is the absolute risk reduction?
What is the relative risk reduction?
It shows heart attack/stroke/death from cardiac causes.
What is the absolute risk reduction?
What is the relative risk reduction?
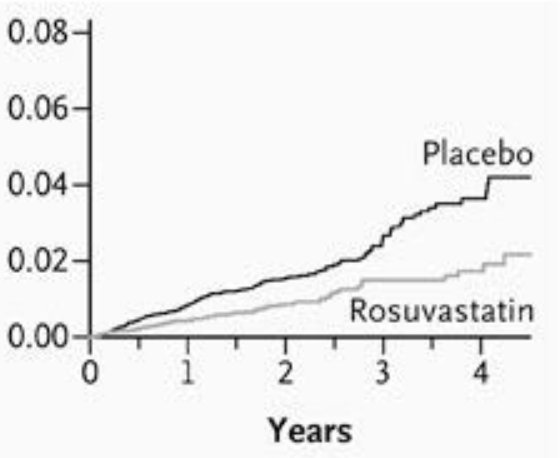
At 4 years, even in the placebo group, 96% of people were absolutely fine.
You could say (and I am sure Aseem would, cheeky chappie that he is!) that they didn't *need* a statin.
But wait!
C50.
At 2 years, what proportion of people "didn't need" a statin?
You could say (and I am sure Aseem would, cheeky chappie that he is!) that they didn't *need* a statin.
But wait!
C50.
At 2 years, what proportion of people "didn't need" a statin?
C51.
At 1 year, what proportion of people "didn't need" a statin, following the same reasoning?
At 1 year, what proportion of people "didn't need" a statin, following the same reasoning?
C52.
Without zooming in, from what you know of similar triangles from above, at 1 month, *roughly* what percentage of patients, "didn't need" a statin?
Without zooming in, from what you know of similar triangles from above, at 1 month, *roughly* what percentage of patients, "didn't need" a statin?
If the world was going to end in 4 years time, and I couldn't easily afford a generic statin, I might skip it. (And spend my money on crisps, computers and curry).
Likewise if I had cancer and 4 years to live.
But this is not the situation my imaginary patient was facing.
Likewise if I had cancer and 4 years to live.
But this is not the situation my imaginary patient was facing.
He, like I, was intending to live into the long future.
When we Brexited away and sunk into the Atlantic.
Or got blown up by an errant tweet from Donald Trump.
His window is not 4 years but 40 years or more.
When we Brexited away and sunk into the Atlantic.
Or got blown up by an errant tweet from Donald Trump.
His window is not 4 years but 40 years or more.
Look at the AREA between the two curves. That is the event free survival. How does the AREA grow with time, during these 4 years?
Hint: Explained in this Seinfeld paper (i.e. paper about nothing) by Tushar Salukhe
circ.ahajournals.org/content/109/15…
Hint: Explained in this Seinfeld paper (i.e. paper about nothing) by Tushar Salukhe
circ.ahajournals.org/content/109/15…
It's about defibrillators, but who cares. Somehow this man turned the bleedin' obvious into a Circulation paper.
If he had discovered DNA, and published that, I wouldn't be impressed - anyone can do that.
But to publish primary school math in Circ - that takes genius!
See pic
If he had discovered DNA, and published that, I wouldn't be impressed - anyone can do that.
But to publish primary school math in Circ - that takes genius!
See pic
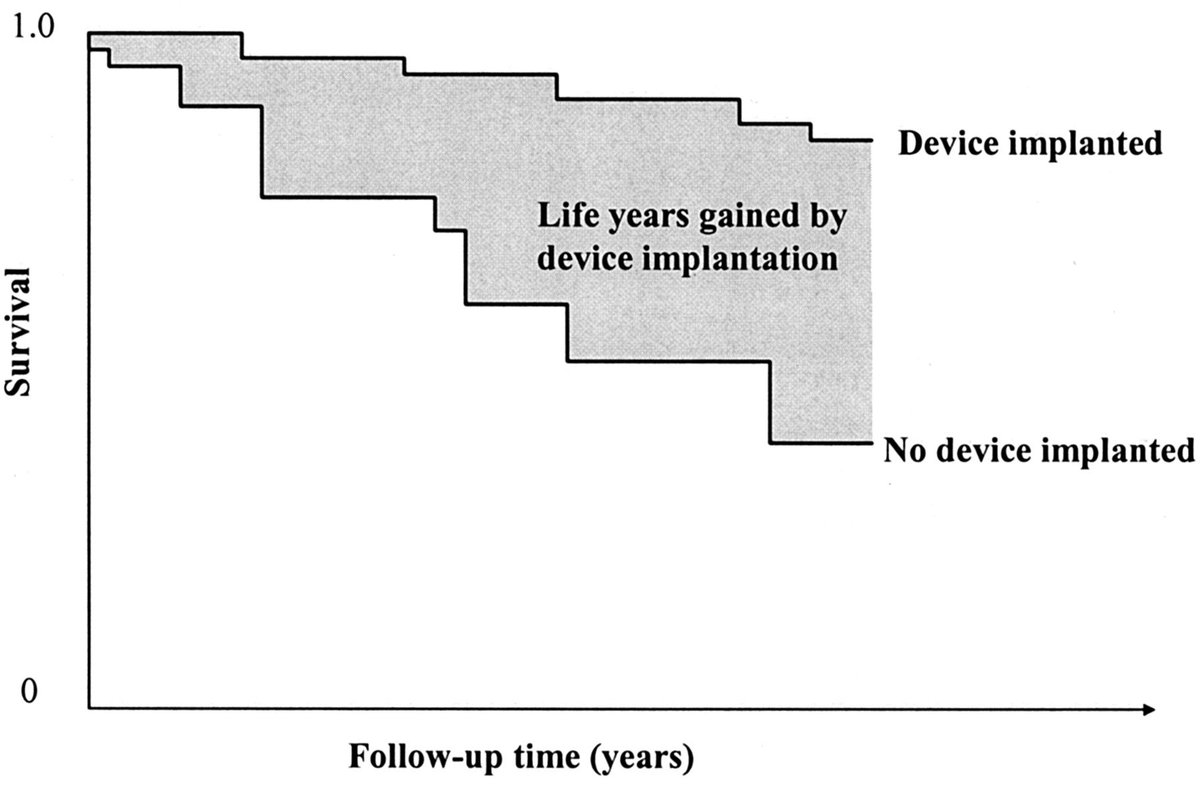
C53.
Start by looking at the left half of the grey triangle. From its top left corner to half way along it.
Then look at the whole grey triangle.
By by what scale factor has its area increased?
Start by looking at the left half of the grey triangle. From its top left corner to half way along it.
Then look at the whole grey triangle.
By by what scale factor has its area increased?
Hmmm. First 3 answers all consistent, but all wrong.
*That* is how Tushar got it into Circ!
It's not as obvious as I thought.
Here is a clue.
Its the new logo for Zygotron Metadynamics (the only bone marrow cardiac stem cell corp you can really trust)
stemcellheartcure.wordpress.com
*That* is how Tushar got it into Circ!
It's not as obvious as I thought.
Here is a clue.
Its the new logo for Zygotron Metadynamics (the only bone marrow cardiac stem cell corp you can really trust)
stemcellheartcure.wordpress.com
Thanks Zainab for alerting me to the attack on this thread by hackers hired by Zygotron Metadynamics in revenge for the release of their new logo. Their lawyers are on to me but have given a useful blog post tip today, that helps answer the question above.
C54
Re-asking because important. Sorry to those who got it right first time: vital to understanding life-years-gained in low risk patients.
Also helpful for passing primary school maths.
View the whole outer triangle, instead of the small top-left small one, does what to area?
Re-asking because important. Sorry to those who got it right first time: vital to understanding life-years-gained in low risk patients.
Also helpful for passing primary school maths.
View the whole outer triangle, instead of the small top-left small one, does what to area?
C55.
Now the Salukhe-Seinfeld question.
If you had a trial, that showed a certain lifespan gain, over its duration, and then you HALVED the duration of the trial, i.e. you looked only at the first half.
What happens to the lifespan gain you will calculate?
Now the Salukhe-Seinfeld question.
If you had a trial, that showed a certain lifespan gain, over its duration, and then you HALVED the duration of the trial, i.e. you looked only at the first half.
What happens to the lifespan gain you will calculate?
C56.
And this single act of looking at just the "left hand half" of the trial duration, does what to the
"Number Needed to Treat, to give One Extra Life Year"
And this single act of looking at just the "left hand half" of the trial duration, does what to the
"Number Needed to Treat, to give One Extra Life Year"
C57.
What is the duration of statin use one is generally *intending* on when one starts?
A few months, see how it goes.
Until a friend get side effects.
Until the first prescription runs out.
Indefinitely.
What is the duration of statin use one is generally *intending* on when one starts?
A few months, see how it goes.
Until a friend get side effects.
Until the first prescription runs out.
Indefinitely.
C58
I see debate here, and neck-and-neck between two answers for a time.
Consider this:
Is cardiovascular risk like pneumonia, where a course of antibiotics cures it?
Or does much of our risk come from things like age, diabetes, family history, weight [in practice hard to ↓]
I see debate here, and neck-and-neck between two answers for a time.
Consider this:
Is cardiovascular risk like pneumonia, where a course of antibiotics cures it?
Or does much of our risk come from things like age, diabetes, family history, weight [in practice hard to ↓]
C59.
In light of this, what is the ideal theoretical length of a trial of primary prevention in LOW RISK (e.g. young and generally normalish) people?
In light of this, what is the ideal theoretical length of a trial of primary prevention in LOW RISK (e.g. young and generally normalish) people?
C60
A 4y trial of 17,000 pts in 1,300 hosps is a landmark.
I am *not* criticising; merely advising how not to misinterpret.
Halving followup approximately quarters lifespan gain.
A 4-year trial instead of 40 years MIGHT underestimate lifespan gain by what factor?
A 4y trial of 17,000 pts in 1,300 hosps is a landmark.
I am *not* criticising; merely advising how not to misinterpret.
Halving followup approximately quarters lifespan gain.
A 4-year trial instead of 40 years MIGHT underestimate lifespan gain by what factor?
Yes, I agree with the majority after 3 votes.
Limiting analysis to 4 years might dramatically underestimate the benefit (in terms of lifespan gain) for low risk pts, because in the first few yrs nothing was going to happen to them.
Other than accumulating coronary atheroma...
Limiting analysis to 4 years might dramatically underestimate the benefit (in terms of lifespan gain) for low risk pts, because in the first few yrs nothing was going to happen to them.
Other than accumulating coronary atheroma...
Aseem has patiently sent me another document in the hope of bamboozling me.
But my bam is not easily boozled.
The article is here jcbmr.com/index.php/jcbm…
I do encourage everyone to read the abstract at least.
But my bam is not easily boozled.
The article is here jcbmr.com/index.php/jcbm…
I do encourage everyone to read the abstract at least.
The article decides to focus on post-2006 RCTs.
These all happen to test one particular statin. Why?
C61
A - Only that one has sufficient patent life for its company to hope for a return on investment
B - It's the weakest statin ever
C - It's the strongest statin ever
These all happen to test one particular statin. Why?
C61
A - Only that one has sufficient patent life for its company to hope for a return on investment
B - It's the weakest statin ever
C - It's the strongest statin ever
C62.
Companies swallow up the easy-to-win indications for a drug, as soon as they can.
Stable angina
Post MI
Acute coronary syndrome
etc.
What was left for the rosuva boys?
A few billion in the bank, but which patient groups left, that others have so far avoided enrolling?
Companies swallow up the easy-to-win indications for a drug, as soon as they can.
Stable angina
Post MI
Acute coronary syndrome
etc.
What was left for the rosuva boys?
A few billion in the bank, but which patient groups left, that others have so far avoided enrolling?
JUPITER covered the low-risk population.
Here are its results
Here are its results
So I am yet again forced to agree with Aseem, although not in the way he probably intended.
Aseem's yellow-highlighted statement is undoubtedly true.
Aseem's yellow-highlighted statement is undoubtedly true.
Thank you so much for your attention.
If you enjoyed this, please retweet the whole quiz-o-rama () to your friends.
If not, send it to your enemies.
If you enjoyed this, please retweet the whole quiz-o-rama () to your friends.
If not, send it to your enemies.
Please reply-tweet with any queries or comments on this quizorama.
Next week I will cover rational management of statin side effects.
If you know anyone (self, friend, pt) who has stopped statins for good because of side effects, we have the solution:
samson-trial.org
Next week I will cover rational management of statin side effects.
If you know anyone (self, friend, pt) who has stopped statins for good because of side effects, we have the solution:
samson-trial.org