In this thread I provide information on inflammation and therapeutic interventions for SARS-CoV2 / COVID-19. The spirit of the thread is to encourage discussion on an important topic in light of numerous clinical interventions (see Figure below). Please read on... 

By now most know the general features of SARS-CoV2 infection and the disease it causes, COVID-19. If not, take a moment to read the Atlantic piece by @edyong209. It is very accessible and is a beautiful piece of writing.
theatlantic.com/science/archiv…
theatlantic.com/science/archiv…
The first job of the immune system is to fight the virus itself. Unfortunately, our immune system has never seen SARS-CoV2 before, so it doesn’t quite know how to behave – like someone drinking alcohol for the first time.
In most individuals, the immune system behaves nicely – a civilized aperitif cocktail. However, in extreme cases the immune system goes berserk – think “Animal House” – and does more damage than the virus itself.
Accumulating evidence suggests that some COVID-19 pts have cytokine storm – and that these patients have poor clinical outcomes: fulminant inflammation can lead to acute respiratory distress syndrome (ARDS), which occurs in up to one-third of patients. thelancet.com/journals/lance…
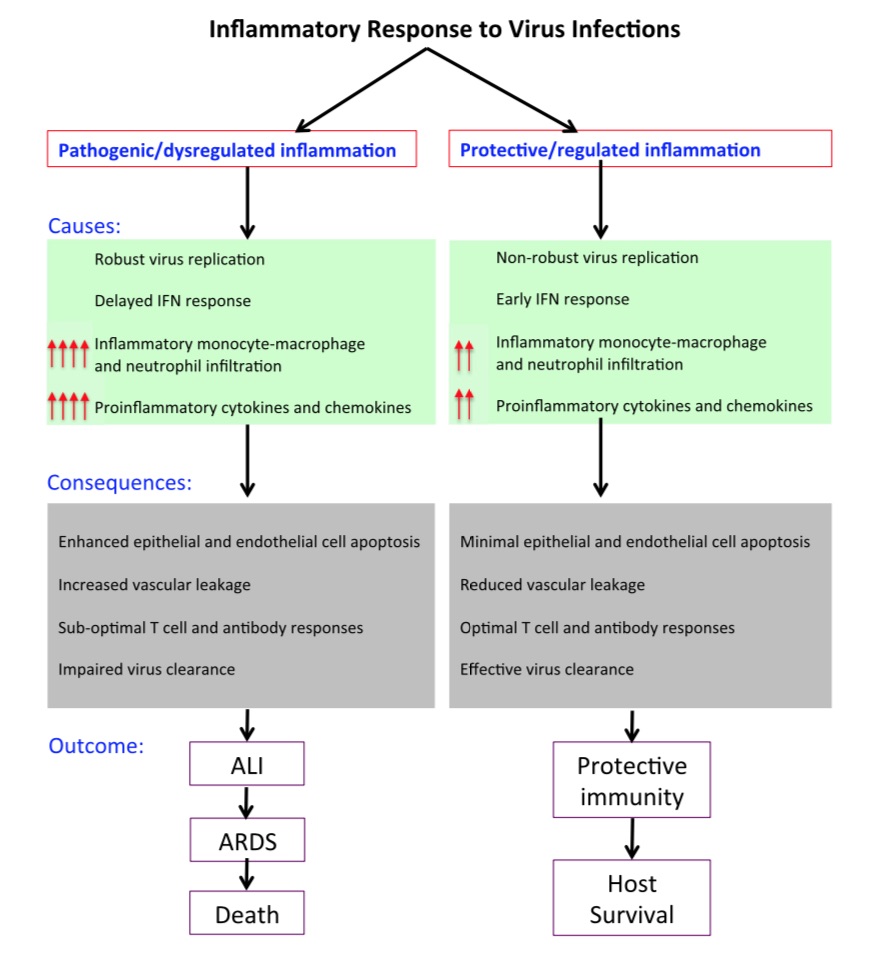
So the challenge is: how does the immune system effectively control the infection early in the clinical course but not lose control in the later stages of disease, resulting in a maladaptive immune response causing ARDS and other complications?
What is the nature of the maladaptive inflammatory response? A picture is emerging, based on (1) related coronaviruses (SARS-CoV, MERS), (2) early evidence from SARS-CoV2/COVID19, and (2) related conditions (e.g., cytokine storm from CAR-T). Here I focus on the first two.
Coronaviruses infecting humans can be classified into low pathogenic hCoVs, which infect the upper respiratory tract, and highly pathogenic CoVs (SARS-CoV [~10% mortality], MERS-CoV [~35% mortality]), which infect the lower resp tract. I will focus on the highly pathogenic CoVs.
Studies of SARS/MERS suggest poor outcomes are due to early events (viral replication leading to high titers, delayed IFN response, infection of diverse airway cells) and late events (accumulation of monocyte-macrophages, neutrophil that secrete cytokines, chemokines).
There is a long list of inflammatory markers that *correlate* with severe disease: cytokines (e.g., IFNg, IL1, IL6, TNF) and chemokines (e.g., CCL2, CXCL10). Unfortunately, it is difficult to know if these are a cause or a consequence of severe disease. It is confusing!

Emerging data in SARS-CoV2/COVID19 suggests that CD4+T lymphocytes are rapidly activated to become pathogenic Th1 cells, and that the cytokines released induce inflammatory CD14+CD16+ monocytes to express IL-6, which accelerates and exacerbates the inflammatory response.
Here are useful references:
ncbi.nlm.nih.gov/pubmed/28466096 ncbi.nlm.nih.gov/pubmed/15030519
doi.org/10.1002/jmv.25…
biorxiv.org/content/10.110…
ncbi.nlm.nih.gov/pubmed/28466096 ncbi.nlm.nih.gov/pubmed/15030519
doi.org/10.1002/jmv.25…
biorxiv.org/content/10.110…
As with SARS/MERS, there is *correlative* data in COVID-19 patients with severe disease: ICU patients had higher plasma levels of IL2, IL7, IL10, GSCF, IP10, MCP1, MIP1A, TNFα, for example. thelancet.com/journals/lance…
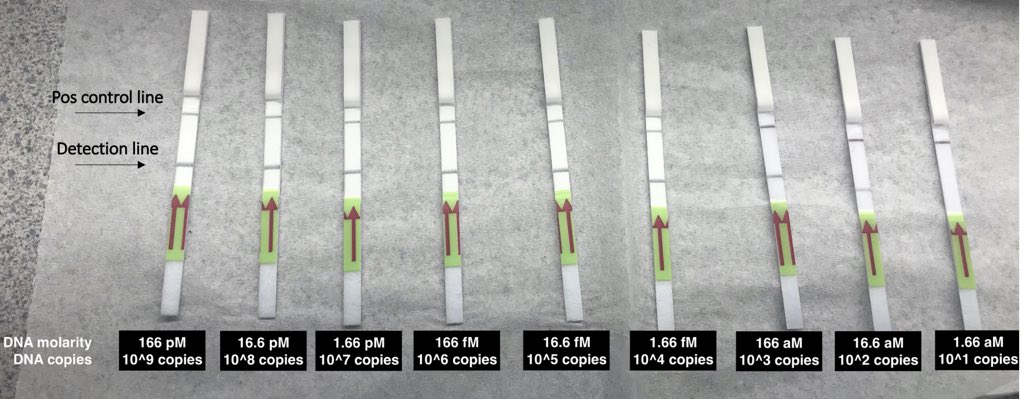
Based on data above, early interventions to *prevent* cytokine storm include direct acting anti-virals that suppress viral replication, antibodies against the virus, interferon (all to reduce viral load) and/or therapeutics that prevent cellular infection/spread (eg, ACE2 decoy).
Late interventions to *treat* cytokine storm include therapies that directly inhibit key inflammatory cytokines (e.g., anti-IL6), inhibit downstream signaling of these cytokines (e.g., JAK inhibitors), and prevent further accumulation of IMMs (which secrete cytokines/chemokines).
An open-label trial with an anti-IL-6 therapy in 21 patients with severe and critical COVID-19 demonstrated suggestive evidence of clinical benefit: symptoms, hypoxygenmia, and CT opacity changes were improved immediately after treatment. chinaXiv:202003.00026v1
Based on the biology above and the small anti-IL6 trial in China, several anti-IL6 trials have been initiated. genengnews.com/news/regeneron…
It is worth noting that anti-IL6 therapy has proven beneficial in CAR-T studies, which may have a similar type of pathogenesis.
But we need more data. We know surprisingly little beyond correlative findings in relatively small samples of COVID-19 patients.
Finally, a disclaimer: like many, I am learning rapidly in this area. I am not a SARS-CoV2/COVID-19 expert. The information here should not be used to guide clinical decisions. I wrote this thread to encourage discussion on an important topic.