Hi hi hi everyone! As Natasha mentioned I'll be talking about healthcare and India. A disclaimer before I start: many of my questions have no answers (yet). There's a lot of information we lack and a lot of research that still needs to be done.
So please feel free to chime in with your own info, perspectives, experiences, and questions! DMs are open if you'd rather stay anonymous and my own twitter handle is @GalatFemme.
A stat to start with: India accounts for 18% of global deaths (that's a LOT!) Out of those 36% are because of communicable diseases, maternal+perinatal conditions, and nutritional deficiencies. Another 53% is because of chronic diseases.
The primary cause of death in India is (no surprise) cardiovascular disease, and the next most common chronic conditions are, in order, COPD, stroke, diabetes, and chronic kidney disease. 
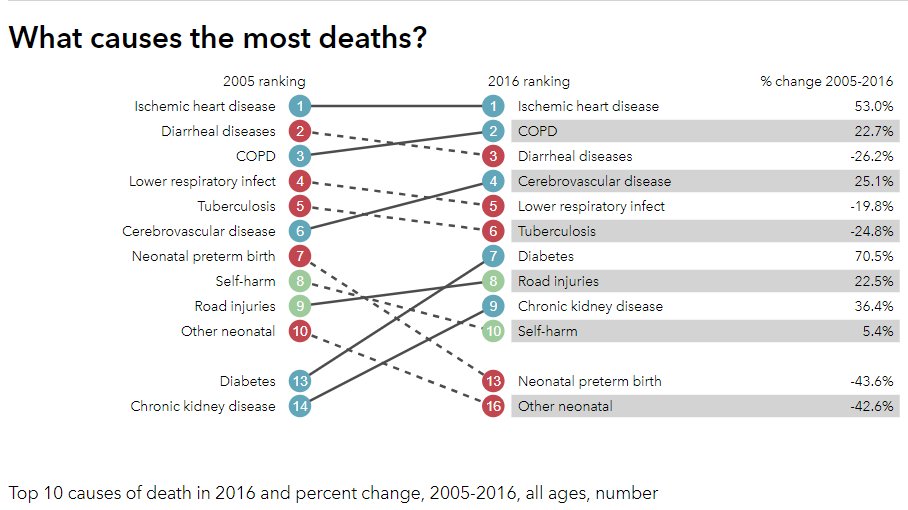
India is commonly referred to as the 'diabetes capital' or having a 'stroke epidemic' - which is true! - but there are some interesting (troubling?) patterns to these diseases.
timesofindia.indiatimes.com/city/ahmedabad…
timesofindia.indiatimes.com/city/ahmedabad…
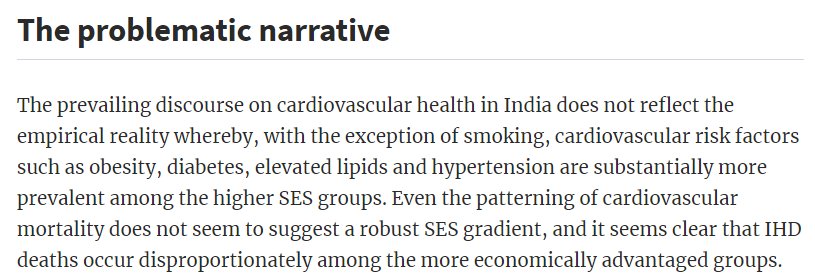
Globally, cardiovascular diseases (CVDs) are generally considered to arise *initially* as 'diseases of affluence' - that is it is first seen in higher economic sections due to poor diet+sedentary lifestyles, and then slowly over a few decades 'reverses' to lower economic sections
The evidence for this is still pretty murky, it hasn't been conclusively proven (or disproved) yet! In India, there's been a increased focus on non communicable diseases (NCDs) of late, especially CVDs, on the supposition that it's no longer just the wealthy who are affected.
However, as this review from 2013 shows, CVD and CVD related deaths are more common in people with higher economic status. The 'reversal' does not seem to have occurred, if it even happens at all.
academic.oup.com/ije/article/42…
academic.oup.com/ije/article/42…
Okay, but a lot of people still suffer from CVD, right? So what's the problem?
Well, this is troubling for a lot of reasons! Mainly we're putting a LOT of resources and attention into conditions that may be only affecting a small portion of the population.
Well, this is troubling for a lot of reasons! Mainly we're putting a LOT of resources and attention into conditions that may be only affecting a small portion of the population.
Although NCDs include a wide variety of diseases, an estimated 63% of papers in India concerning chronic non communicable diseases are about cardiovascular conditions. Other conditions in India very often get little or no attention, possibly due to lack of funding?
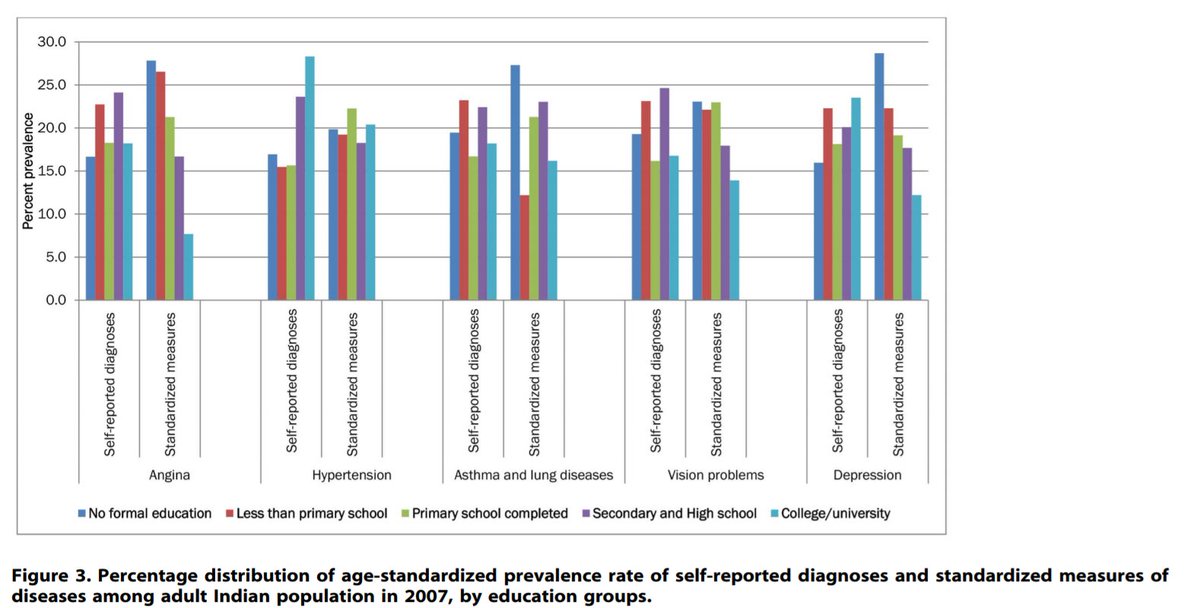
Something else to think about is how reliable this data is. According to this paper from 2013, higher and lower economic groups are equally affected by CVDs. The problem is getting everyone diagnosed.
ncbi.nlm.nih.gov/pmc/articles/P…
ncbi.nlm.nih.gov/pmc/articles/P…
One clear difference between higher and lower socioeconomic groups is getting access to information, healthcare, and accurate diagnoses. When asked to self report diagnosis and then being tested, people of lower income groups almost always UNDER reported their conditions...

...while people of higher income groups always OVER reported their conditions! Very similar figures are seen with levels of education.
An obvious conclusion is that wealthier, more educated people are more likely to recognise and seek help for their chronic NCDs.
An obvious conclusion is that wealthier, more educated people are more likely to recognise and seek help for their chronic NCDs.
'One Disability-Adjusted Life Year can be thought of as one lost year of "healthy" life' - from the WHO site.
NCDs account for about 44% of DALY in India. The brunt of living with disabilities is then borne by lower economic sections, many of whom are never even diagnosed.
NCDs account for about 44% of DALY in India. The brunt of living with disabilities is then borne by lower economic sections, many of whom are never even diagnosed.
Chronic NCDs are often treatable but as pointed out, they are underdiagnosed, or diagnosed too late, and medical care is often too costly or even inaccessible for most people.
"Health expenditures are responsible for more than half of Indian households
falling into poverty; the impact of this has been increasing pushing around 39 million Indians into poverty each year."
Source: (2011) ncbi.nlm.nih.gov/pmc/articles/P…
falling into poverty; the impact of this has been increasing pushing around 39 million Indians into poverty each year."
Source: (2011) ncbi.nlm.nih.gov/pmc/articles/P…
India is often held up as a example of the 'Double Burden' - having both diseases of affluence and diseases of poverty - but the weight of each is rarely mentioned and definition of double burden itself is debatable. Are we allocating resources proportional to the burden?
The inverse care law says that those with the greatest need for health care have the greatest difficulty in accessing health services and are least likely to have their health needs met.
Yuuup, sounds about right 😕
Yuuup, sounds about right 😕
Speaking of access, while India meets the global average for number of doctors, 74% of our doctors cater to only one third of the urban population.
firstpost.com/india/indias-h…
firstpost.com/india/indias-h…
A large portion of major NCDs remain undiagnosed in rural areas. Even once diagnosed, an estimated 12% go untreated, compared to only 3% left untreated in urban areas - four times as many!
The disparities only get worse when factoring in other aspects like caste and tribe. Scheduled castes are turned away by government staff or asked for exorbitant bribes.
scroll.in/article/884644…
scroll.in/article/884644…
A whole ONE FIFTH of major diagnosed disease remain untreated among scheduled tribes and many more are never diagnosed. Public primary health centres are facing a shortage of doctors that only keeps increasing, meaning long journeys to private health centres and higher costs.
It's not surprising that India has one of the lowest per capita healthcare expenditures in the world. The government contributes only 32% to insurance. The majority of Indians (76%) do not have insurance and end up having to pay for everything themselves.
The burden of healthcare costs is also disproportionately higher on lower economic groups! Poor households spend an average of 15% of their monthly income on healthcare compared to richer households that pay <1% of their monthly income!
The differences between rural and urban health care don't end with understaffing. Two aspects of medical professionals influence the quality of care provided: competence and effort. Doctors in the public sector are often better qualified and more competent than in private sector
..but *they expend LESS effort with patients from a rural/lower economic background* and as mentioned are often turned away for casteist reasons. Patients are the forced to avail of private facilities where doctors are LESS qualified and more expensive!
bit.ly/2vkqhQd
bit.ly/2vkqhQd
One reason is that wealthier/well educated patients have more information at their disposal and are able to advocate for themselves (sometimes leading to doctors overdoing it by prescribing unnecessary drugs). Another is that doctors are poorly compensated and lack incentives.
Data from the National Rural Health Mission (NRHM)'S 11th Plan (2007-2012) show that 90% of the resources allocated for health was spent on family welfare programs (i.e. family planning) and only 7.7% for disease control. The 12th (and last) Plan tripled spending on health.
Professional malpractice, corruption, fudging records, and healthcare fraud are common. Disturbingly whistle blowers often lose their jobs or even end up dead.
reuters.com/article/us-ind…
reuters.com/article/us-ind…
Verbal or physical assaults have been reported by up to 75% of hospital staff across the country. An overburdened and ill managed healthcare system is failing its patients and doctors both.
Interestingly medical tourism is booming. Uninsured Americans struggling to afford medical aid find quality care at a fraction of the cost in private hospitals in India. 'Medical visas', introduced in 2005 are steadily increasing (1,70,000 issued in 2016)
foreignpolicy.com/2018/01/02/ind…
foreignpolicy.com/2018/01/02/ind…
But what does this mean for us?
On the one hand, it is a source of revenue that could help our badly underfunded public health sector! Unfortunately there is no evidence that any of that money actually makes its way back to the institutions that need it.
On the one hand, it is a source of revenue that could help our badly underfunded public health sector! Unfortunately there is no evidence that any of that money actually makes its way back to the institutions that need it.
The central government offers land at concessional rates to private hospitals in return for 10% of inpatient and 25% of outpatient being provided free to low socioeconomic status groups. However many private hospital openly disregard these rules and wriggle out of paying fines.
Instead the medical tourism industry is more likely to attract doctors into the private sector leaving the public sector even more overloaded. In short, catering to the (relatively) wealthier Americans, would probably make our existing socioeconomic divide wider and wider.