,
30 tweets,
7 min read
Read on Twitter
MYOCARDIAL VIABILITY
================
Lazarus revisited
[Tweetorial from ORBITA-hq: "Making cardiologists think again"(TM)]
Please retweet to cardiology fellows or anyone who might be interested to practice data interpretation.
================
Lazarus revisited
[Tweetorial from ORBITA-hq: "Making cardiologists think again"(TM)]
Please retweet to cardiology fellows or anyone who might be interested to practice data interpretation.

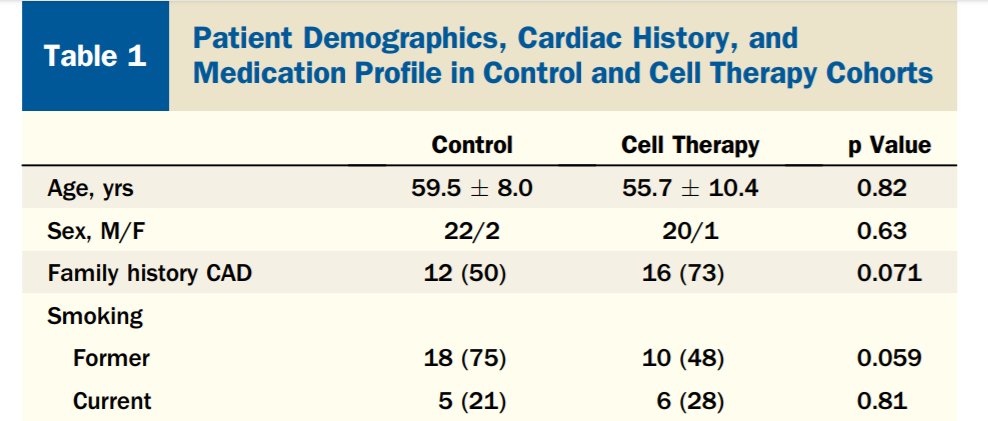
Let's start our story here, when I was first informed that viability testing saves lives.
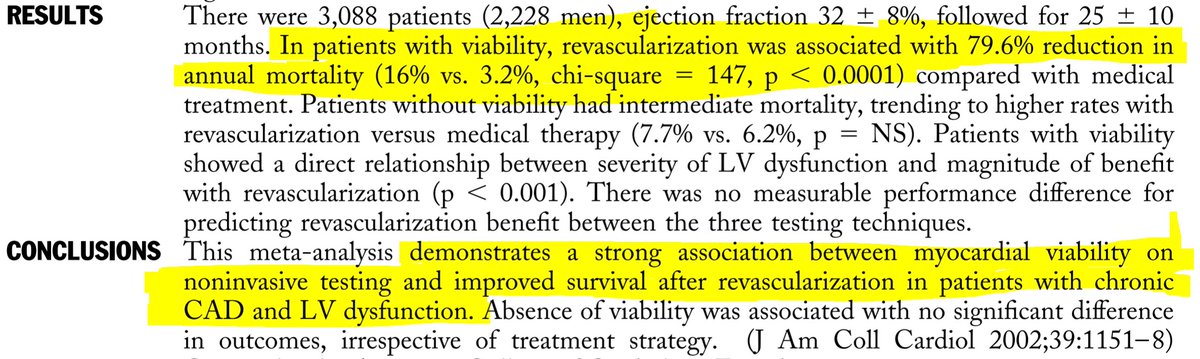
A few weeks later, a decisive meta-analysis.
3000 patients
3000 patients
... whose primary result figure soon became the MOST SHOWN figure in lectures on viability.
Within 2 years I had seen it perhaps a dozen times, in lectures across the world, to prove the unassailable merit of viability testing.
Here it is. Fall backwards in awe ye skeptics.
Within 2 years I had seen it perhaps a dozen times, in lectures across the world, to prove the unassailable merit of viability testing.
Here it is. Fall backwards in awe ye skeptics.
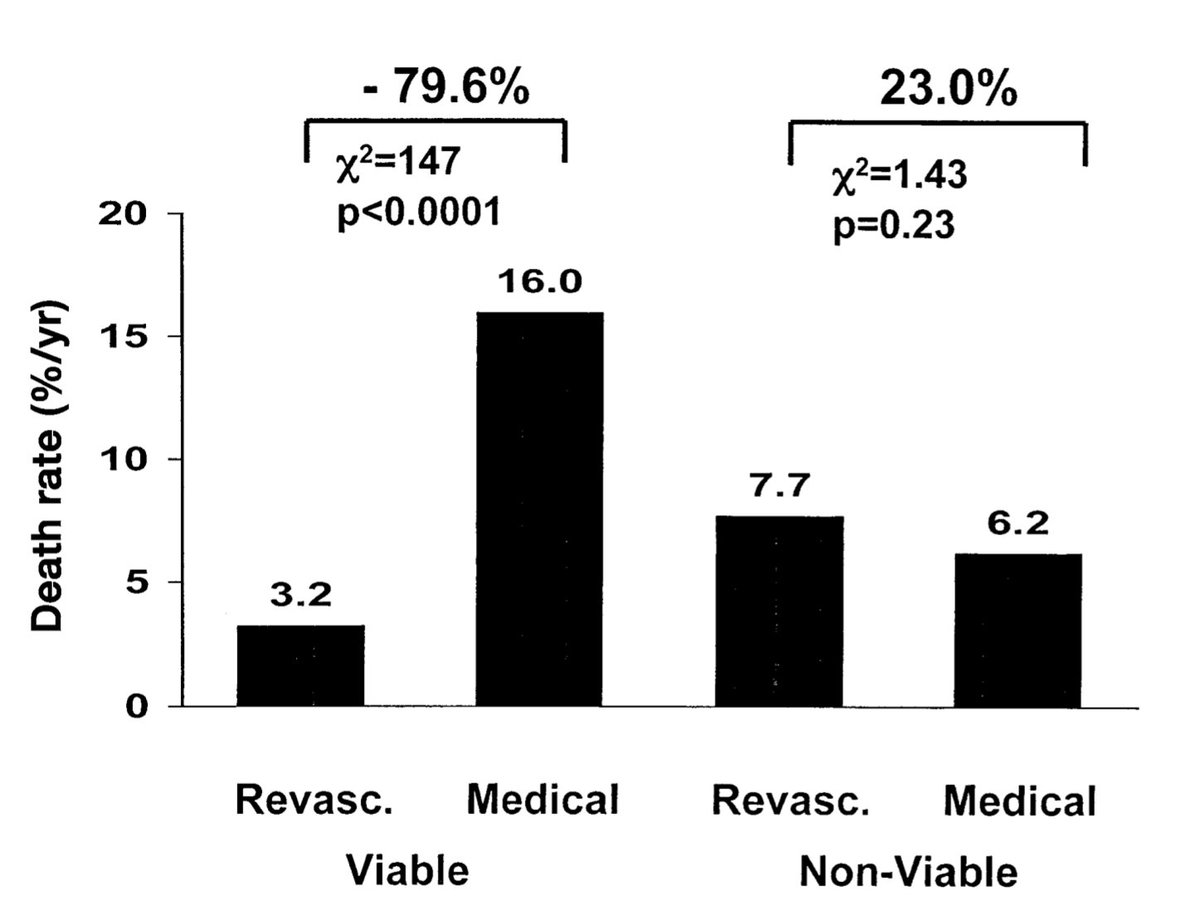
From this LANDMARK figure, what do tweeps on #cardiotwitter #meded #foamed infer?
(Please answer: this subject is at the expense of the #ORBITA-ACME shootout, making Anish Koka unhappy.)
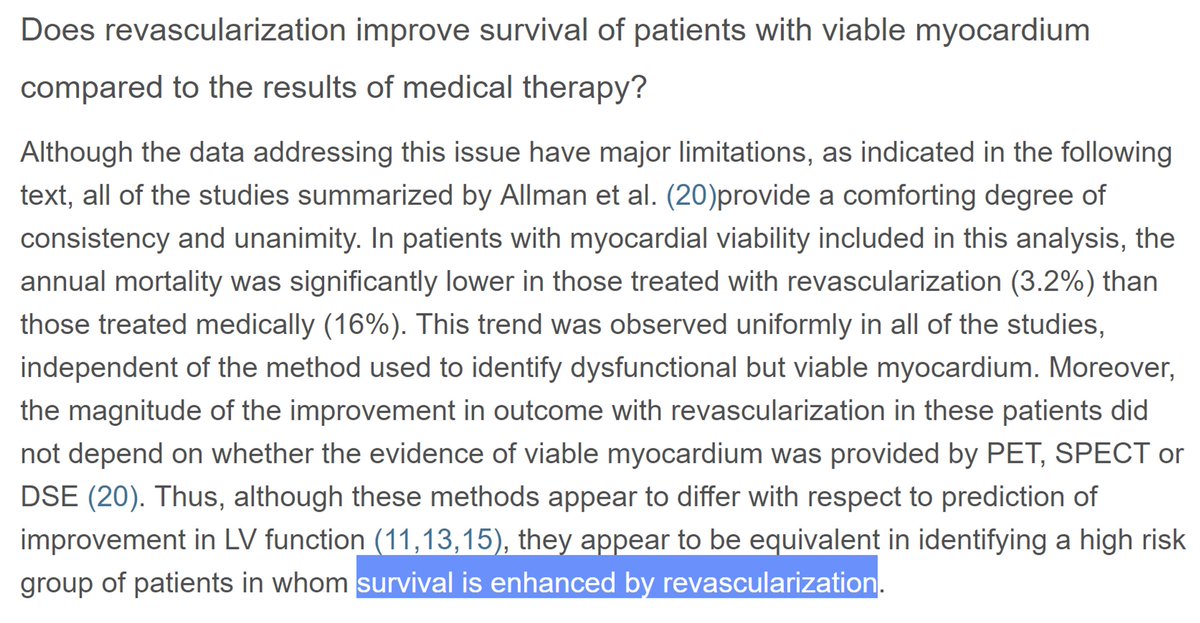
If I have a patient WITH viable myocardium, revasc'ing them does what to annual mortality?
(Please answer: this subject is at the expense of the #ORBITA-ACME shootout, making Anish Koka unhappy.)
If I have a patient WITH viable myocardium, revasc'ing them does what to annual mortality?
Does it help to have the legend to this LANDMARK figure?

And another landmark figure, Bob Bonow, provides this editorial to help readers understand the magnitude of the news.
Remember the only reason I am doing this stuff is because people respond to the quizzes. I am very grateful for your involvement.
The first 4 answers show why this sort of data interpretation practice is so needed.
The first 4 answers show why this sort of data interpretation practice is so needed.
I am a cardiology trainer and every week have a few meetings with Cardiology fellows from across London for advice etc. Many have seen these tweetorials and said useful (of course! I am their boss!)
They have two feelings about them.
They have two feelings about them.
(A) "I hate them. I keep getting them wrong. Your question on X was particularly evil. I thought the answer was Y, but it was Z."
(B) "Oh they are very good, thank you for doing them. A great help!"
"Did you get many wrong?"
"Well I didn't vote, I didn't want to look stupid"
(B) "Oh they are very good, thank you for doing them. A great help!"
"Did you get many wrong?"
"Well I didn't vote, I didn't want to look stupid"
Without exception, amongst those that have come across them, the trainees coming to announce progress in their careers, discuss their PhD plans, etc, are in group (A).
Those who are struggling, worried or are sent to see me because others are worried, are in (B).
Those who are struggling, worried or are sent to see me because others are worried, are in (B).
Moral:
If you want to learn, commit to an answer. NOBODY knows what you voted.
If right, shout Hooray.
If wrong, shout, "Double Hooray - I've learned something; many days go by where I don't."
If don't agree wrong, DM me, as you will not be the only one. (And I may be wrong!)
If you want to learn, commit to an answer. NOBODY knows what you voted.
If right, shout Hooray.
If wrong, shout, "Double Hooray - I've learned something; many days go by where I don't."
If don't agree wrong, DM me, as you will not be the only one. (And I may be wrong!)
At 7 votes, I can see the winner so far is a neck-and-neck tie between "Revasc reduces mort by 79.6%" and "Revasc reduces mort by 12.8%".
How can two such different figures both be equally right?
Let's do a thought experiment!
How can two such different figures both be equally right?
Let's do a thought experiment!
*IMAGINE* I randomize 2000 patients into two arms:
1000 patients go into the BARTTELS arm of good stuff
The other 1000 draw the short straw, they get @richardbogle BOGLED.
Just 32 patients die with BARTTELS
A whopping 160 patients die under BOGLING
1000 patients go into the BARTTELS arm of good stuff
The other 1000 draw the short straw, they get @richardbogle BOGLED.
Just 32 patients die with BARTTELS
A whopping 160 patients die under BOGLING

Thanks to BOGLING, there have been 160, not 32, deaths.
Richard Bogle dutifully attends all 160 funerals of his patients. Keeps him busy that year (2017).
Just about now he is thinking to himself:
"How many of these funerals could I have avoided if I had only BARTTELed?"
Richard Bogle dutifully attends all 160 funerals of his patients. Keeps him busy that year (2017).
Just about now he is thinking to himself:
"How many of these funerals could I have avoided if I had only BARTTELed?"
ask him for a percentage for a news story. How to calc percentage?
Divide by something, and mult by 100%. But divide by what?
Divide by 160 (the number of funerals he attended)?
Or divide by 1000, (the potential number of funerals he may have had to attend)
Divide by something, and mult by 100%. But divide by what?
Divide by 160 (the number of funerals he attended)?
Or divide by 1000, (the potential number of funerals he may have had to attend)
That's the choice we have between RELATIVE risk reduction and ABSOLUTE.
RELATIVE means as a proportion of how many deaths in the OTHER ARM.
ABSOLUTE means as a proportion of how many PATIENTS YOU HAD ALTOGETHER in your arm.
What is the RELATIVE risk reduction of BARTTELSing?
RELATIVE means as a proportion of how many deaths in the OTHER ARM.
ABSOLUTE means as a proportion of how many PATIENTS YOU HAD ALTOGETHER in your arm.
What is the RELATIVE risk reduction of BARTTELSing?
What is the ABSOLUTE risk reduction of BARTTELSing?
RELATIVE risk reductions tend to be more conserved across different risk groups and durations.
Statin trials for event prevention show this elegantly with 10s of thousands of randomized patients
(If not tried, please have a go at the statin tweetorial
)
Statin trials for event prevention show this elegantly with 10s of thousands of randomized patients
(If not tried, please have a go at the statin tweetorial
)
Yet while relative risk reductions help us compare trials:
What matters to patients is ABSOLUTE risk reductions. If deaths are rare, even (say) halving them, doesn't actually prevent many of the PATIENTS TREATED from dying.
"If you're not going to die, I can't save your life."
What matters to patients is ABSOLUTE risk reductions. If deaths are rare, even (say) halving them, doesn't actually prevent many of the PATIENTS TREATED from dying.
"If you're not going to die, I can't save your life."
The RELATIVE reductions are not wrong, they just need to be taken into the context of the patient and their time window.
Beware that for chronic conditions, the ABSOLUTE is heavily dependent on the time window. Over a short time, the ABSOLUTE benefit of (say) ACEi for HF is tiny
Beware that for chronic conditions, the ABSOLUTE is heavily dependent on the time window. Over a short time, the ABSOLUTE benefit of (say) ACEi for HF is tiny
Let's exit the thought experiment re BARTTELS and BOGLE.
Please note that Richard Bogle has been my friend for about 2 decades. We trained together and I frequently wind him up, although I haven't seen him in person for over 10 years.
Back to the miracle of viability.
Reminder:
Please note that Richard Bogle has been my friend for about 2 decades. We trained together and I frequently wind him up, although I haven't seen him in person for over 10 years.
Back to the miracle of viability.
Reminder:
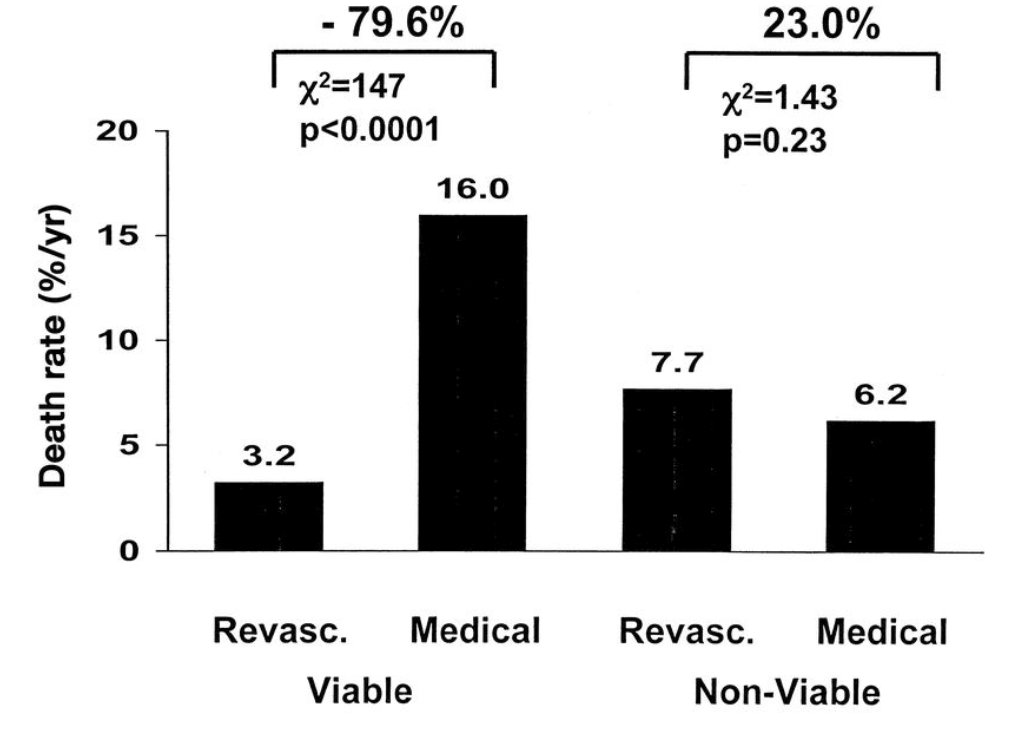
Of those who have been to lectures on viability/hibernation/whatnot, how many of you have seen that figure above presented?
The commonest conclusion presented by a lecturer is that
"This 3000 patient meta analysis shows that:
(A) In viable myocardium, revasc improves survival 79.6%.
(B) In non-viable myocardium, revasc doesn't help survival significantly."
What do you think of (A)?
"This 3000 patient meta analysis shows that:
(A) In viable myocardium, revasc improves survival 79.6%.
(B) In non-viable myocardium, revasc doesn't help survival significantly."
What do you think of (A)?
What do you think of (B)?
Thank you!
Based on the above meta-analysis of 3000 patients, what is your best estimate of the RELATIVE RISK REDUCTION in cardiac mortality?
If you did a single, well-conducted, carefully-controlled randomized controlled trial, what RRR would you expect?
Based on the above meta-analysis of 3000 patients, what is your best estimate of the RELATIVE RISK REDUCTION in cardiac mortality?
If you did a single, well-conducted, carefully-controlled randomized controlled trial, what RRR would you expect?
Come on, this is not difficult 8-)
We do meta analyses of smaller studies to help estimate the effect size of what a single larger study would show.
So just use your previous estimate of the RELATIVE risk reduction.
No trick here.
So just use your previous estimate of the RELATIVE risk reduction.
No trick here.
Can i have 10 votes please? Otherwise I think everyone has died and I am the last person on earth. Zombie apocalypse.
If your thread stops here, continue by clicking below: