Starting a series on clinical Pearls I am gathering in #COVID19 patients based on experiences of many experts
Will add as we go along
Feel free to add your own observations/experiences
#covidclinicalpearls /1
Will add as we go along
Feel free to add your own observations/experiences
#covidclinicalpearls /1
Anosmia is likely the most specific #COVID19 related symptom
30% of patients have anosmia as their 1st symptom
#covidclinicalpearls /2
30% of patients have anosmia as their 1st symptom
#covidclinicalpearls /2
Around 90% of patients have fever.
50% maybe afebrile at the time of presentation
Fever tends to be very resistant to routine measures in hospitalized patients
There is no consensus that NSAIDs are to be avoided in #COVID2019 patients
#covidclinicalpearls /3
50% maybe afebrile at the time of presentation
Fever tends to be very resistant to routine measures in hospitalized patients
There is no consensus that NSAIDs are to be avoided in #COVID2019 patients
#covidclinicalpearls /3
Viral shedding is greatest at the time of symptom onset and declines over the course of several days
50% of patients keep shedding after complete resolution of symptoms
Viral shedding can continue for as much as 24 days
#COVID2019
#covidclinicalpearls /4
50% of patients keep shedding after complete resolution of symptoms
Viral shedding can continue for as much as 24 days
#COVID2019
#covidclinicalpearls /4
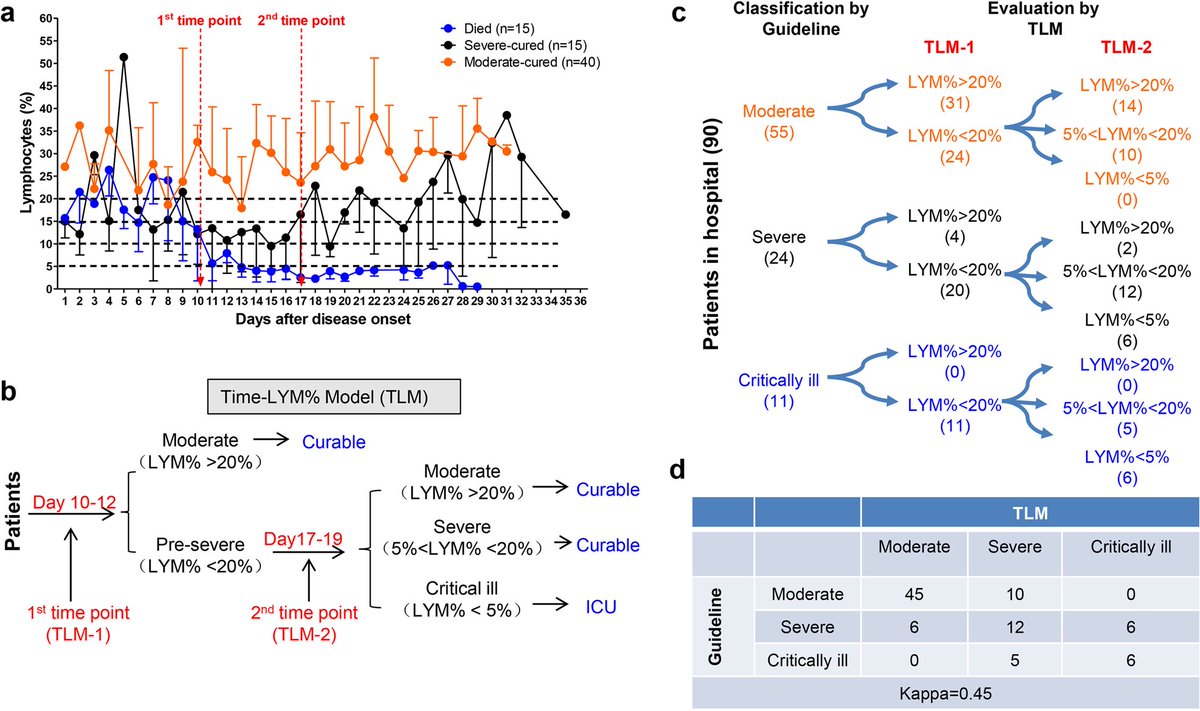
Lymphopenia is common in #COVID2019 > 80% patients
Leukopenia is seen in 1/3 of patients
Its associates with poor outcomes and poor surivival.
Recovery with Lym % > 20% at Day10 of symptoms is a + outcome marker
Lym % of <5% = poor prognosis
#covidclinicalpearls /5
Leukopenia is seen in 1/3 of patients
Its associates with poor outcomes and poor surivival.
Recovery with Lym % > 20% at Day10 of symptoms is a + outcome marker
Lym % of <5% = poor prognosis
#covidclinicalpearls /5
Lymphopenia timeline in #COVID19
LYM% < 20% are pre-severe type
At TLM-2
If LYM% > 20% those are reclassified as “moderate”
If 5% < 20% = “severe”
If < 5% = “critical”
#covidclinicalpearls /6
LYM% < 20% are pre-severe type
At TLM-2
If LYM% > 20% those are reclassified as “moderate”
If 5% < 20% = “severe”
If < 5% = “critical”
#covidclinicalpearls /6
Diagnosis by PCR testing has upto 30% false negative rate #COVID19
Sampling early in disease course will have lower sensitivity
CT Chest has BETTER predictive value in cases where CT findings are high probability even if PCR swab negative
#covidclinicalpearls /7
Sampling early in disease course will have lower sensitivity
CT Chest has BETTER predictive value in cases where CT findings are high probability even if PCR swab negative
#covidclinicalpearls /7
Average time from initial negative to positive PCR swab test is 5 days
Do NOT rule out #COVID19 with ONE pharyngeal swab.
Sensitivity of CT in patients with positive CT & negative PCR is 97%
#covidclinicalpearls /8
Do NOT rule out #COVID19 with ONE pharyngeal swab.
Sensitivity of CT in patients with positive CT & negative PCR is 97%
#covidclinicalpearls /8
#CT Chest in #COVID19
Early #groundglass abnormality in early disease,
followed by “crazy paving,”
finally increasing consolidation
Typically peripheral
#covidclinicalpearls /9
Early #groundglass abnormality in early disease,
followed by “crazy paving,”
finally increasing consolidation
Typically peripheral
#covidclinicalpearls /9
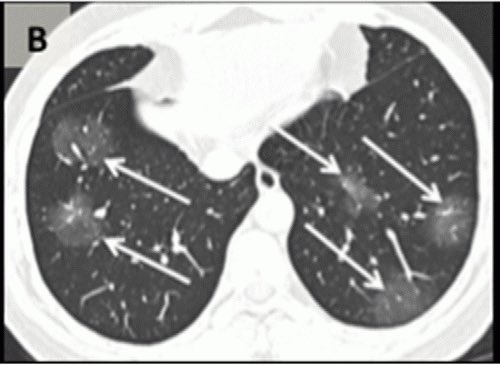

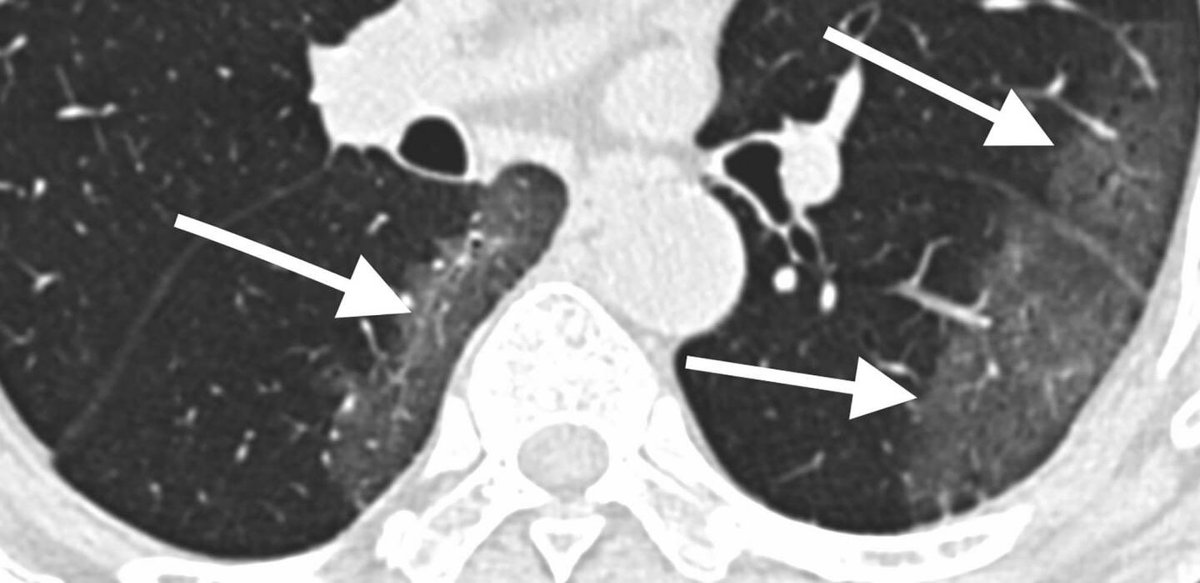
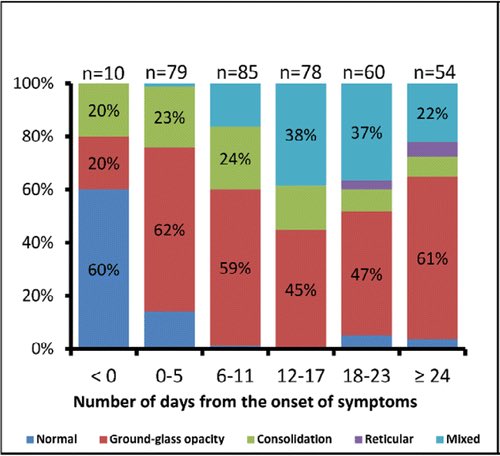
Temporal changes of CT findings in #COVID19
Note #groundglass predominant early
#covidclinicalpearls /10
Note #groundglass predominant early
#covidclinicalpearls /10
Respiratory support
#COVID19
AVOID
- Noninvasive ventilations #NPPV
- High flow O2 #HFNC
due to high risk to healthcare workers due to aerosols.
EARLY intubation
#covidclinicalpearls /11
#COVID19
AVOID
- Noninvasive ventilations #NPPV
- High flow O2 #HFNC
due to high risk to healthcare workers due to aerosols.
EARLY intubation
#covidclinicalpearls /11
For #intubation in #COVID19
Only Experts intubate
AVOID bag-mask ventilations
Use PEEP valve if needed
Gentle bagging via supraglottic device preferred if needed
Always use rapid sequence intubation - rocuronium preferred by some
#covidclinicalpearls /12
Only Experts intubate
AVOID bag-mask ventilations
Use PEEP valve if needed
Gentle bagging via supraglottic device preferred if needed
Always use rapid sequence intubation - rocuronium preferred by some
#covidclinicalpearls /12
If using #NPPV #NIV in #COVID2019 (#Ventilator in short supply)
Use a full face mask or helmet
Use a filter for the leak port
Use a HME Filter to provide additional safety from aerosol
Set Alarms for patient disconnect
#covidclinicalpearls /13
Use a full face mask or helmet
Use a filter for the leak port
Use a HME Filter to provide additional safety from aerosol
Set Alarms for patient disconnect
#covidclinicalpearls /13
If using #HFNC (preferred to #NIV) in #COVID19
Use preferably low flow rates (30-40L/min) have lower rates of aerosolization
Always increase FiO2 to max before increasing flow rate >30L/min
Reassess at 1 hr and 3 hr intervals for possible intubation
#covidclinicalpearls /14
Use preferably low flow rates (30-40L/min) have lower rates of aerosolization
Always increase FiO2 to max before increasing flow rate >30L/min
Reassess at 1 hr and 3 hr intervals for possible intubation
#covidclinicalpearls /14
Use of Venturi mask
#COVID19
if patient requires >8L/min NC
Non humidified
Uptitrate to FiO2 35%
Then increase flow rate if needed to 12 L/min
#covidclinicalpearls /15
#COVID19
if patient requires >8L/min NC
Non humidified
Uptitrate to FiO2 35%
Then increase flow rate if needed to 12 L/min
#covidclinicalpearls /15
For mechanical #ventilation in #COVID19 #ICU
Tidal volume 6ml/kg IBW
PEEP 5 if BMI <35
(10 if BMI >35)
Avoid HIGH PEEP
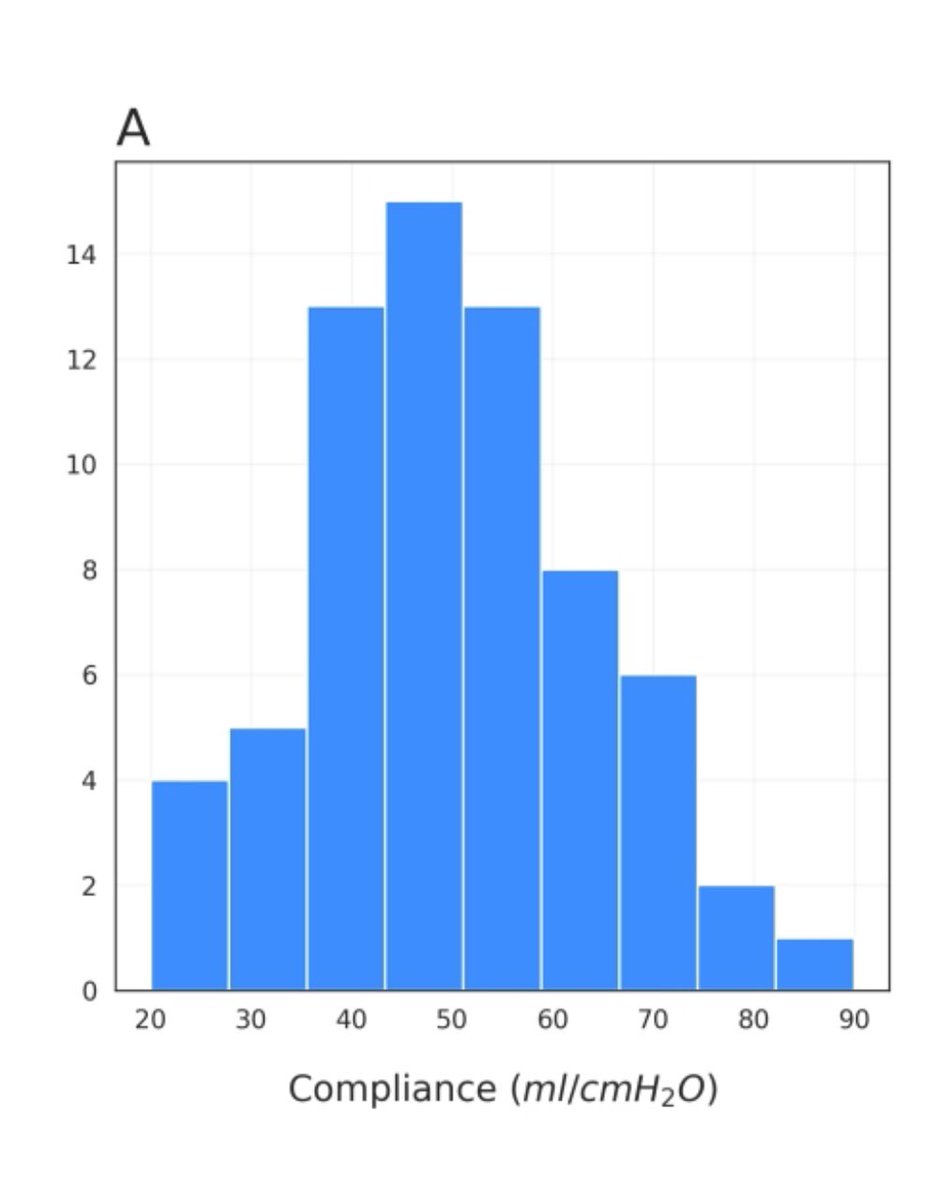
#COVID19 ARDS is atypical with normal compliance & high PEEP may do more harm than good
#covidclinicalpearls /16
Tidal volume 6ml/kg IBW
PEEP 5 if BMI <35
(10 if BMI >35)
Avoid HIGH PEEP
#COVID19 ARDS is atypical with normal compliance & high PEEP may do more harm than good
#covidclinicalpearls /16
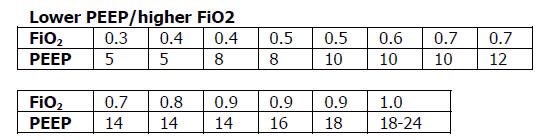
Use ARDSnet LOW PEEP table as a guide but try to maintain as low a PEEP as feasible early in #COVID19 disease
#covidclinicalpearls /17
#covidclinicalpearls /17
#COVID19 #ARDS is atypical
Compliance tends to normal-high
Hence high PEEP strategy may not improve oxygenation
#covidclinicalpearls / 17
Compliance tends to normal-high
Hence high PEEP strategy may not improve oxygenation
#covidclinicalpearls / 17
#proning #prone #ventilation in #COVID19 #ARDS
General consensus is to prone early
Suggest prone ventilation in non-intubated patients in early lung injury
Awake patient may lie in prone position for 12-16hrs a day
#covidclinicalpearls /18
General consensus is to prone early
Suggest prone ventilation in non-intubated patients in early lung injury
Awake patient may lie in prone position for 12-16hrs a day
#covidclinicalpearls /18
#proning in #COVID19
#ARDS
Prone positioning of patients with relatively high compliance results in a modest benefit at the price of a high demand for stressed human resources
Be judicious and reassess benefits of prone #ventilation
#covidclinicalpearls /19
#ARDS
Prone positioning of patients with relatively high compliance results in a modest benefit at the price of a high demand for stressed human resources
Be judicious and reassess benefits of prone #ventilation
#covidclinicalpearls /19
#COVID19 #ARDS
High reintubation rates
Glottic edema/stridor common after extubation
Leak test before extubation is critical
Delayed extubation (longer than typical) may help extubation failures
#covidclinicalpearls /20
High reintubation rates
Glottic edema/stridor common after extubation
Leak test before extubation is critical
Delayed extubation (longer than typical) may help extubation failures
#covidclinicalpearls /20
#COVID19 #ARDS
Nitric oxide has anti viral effect invitro
Initiate iNO in refractory cases at 20ppm
If repeat ABG in 2 hrs PaO2 ⬆️10% continue - if not ⬆️iNO to 80ppm - if still no ⬆️PaO2 stop
Alternative consider #epoprostenol
#covidclinicalpearls /21
Nitric oxide has anti viral effect invitro
Initiate iNO in refractory cases at 20ppm
If repeat ABG in 2 hrs PaO2 ⬆️10% continue - if not ⬆️iNO to 80ppm - if still no ⬆️PaO2 stop
Alternative consider #epoprostenol
#covidclinicalpearls /21
#Covid_19 UK group reports wedge infarcts/pulmonary thrombosis & prevalence of pulmonary embolism.
Role for Anticoagualtion?
In patients with coagulopathy or D Dimer >6X high use of LMWH was associated with reduced mortality (40% vs 64%)
#COVID19
#covidclinicalpearls /22
Role for Anticoagualtion?
In patients with coagulopathy or D Dimer >6X high use of LMWH was associated with reduced mortality (40% vs 64%)
#COVID19
#covidclinicalpearls /22
#ECMO
in #Covid_19
It’s “rarely necessary”
Several concerns for use - including potential for lymphopenia and worse outcomes
Very limited role /if any
#covidclinicalpearls /23
in #Covid_19
It’s “rarely necessary”
Several concerns for use - including potential for lymphopenia and worse outcomes
Very limited role /if any
#covidclinicalpearls /23
#fluidmanagement in #COVID19
Do NOT give routine 30cc/kg resuscitation IVF
Restrict Fluids
Limit use of maintenance IVF
Do not use ⬆️Lactate to trigger IVF
Avoid diuretic use (—> AKI)
Avoid large + fluid balance
#covidclinicalpearls /24
Do NOT give routine 30cc/kg resuscitation IVF
Restrict Fluids
Limit use of maintenance IVF
Do not use ⬆️Lactate to trigger IVF
Avoid diuretic use (—> AKI)
Avoid large + fluid balance
#covidclinicalpearls /24
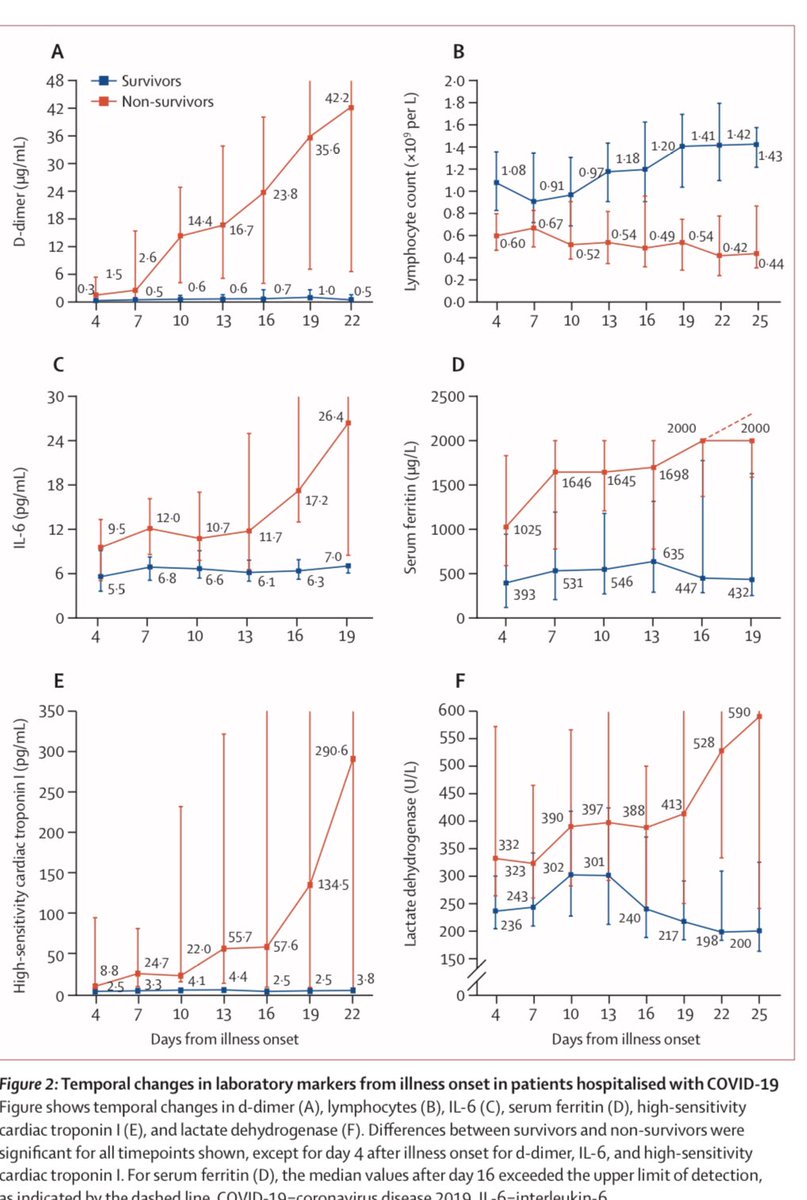
#troponin in #Covid_19
Increase rapidly from D14
Steady rise from D4 to D22 is seen in non survivors
Fulminant myocarditis has been described
Cardiogenic shock important cause of death ~30% of deaths
#covidclinicalpearls /25
Increase rapidly from D14
Steady rise from D4 to D22 is seen in non survivors
Fulminant myocarditis has been described
Cardiogenic shock important cause of death ~30% of deaths
#covidclinicalpearls /25
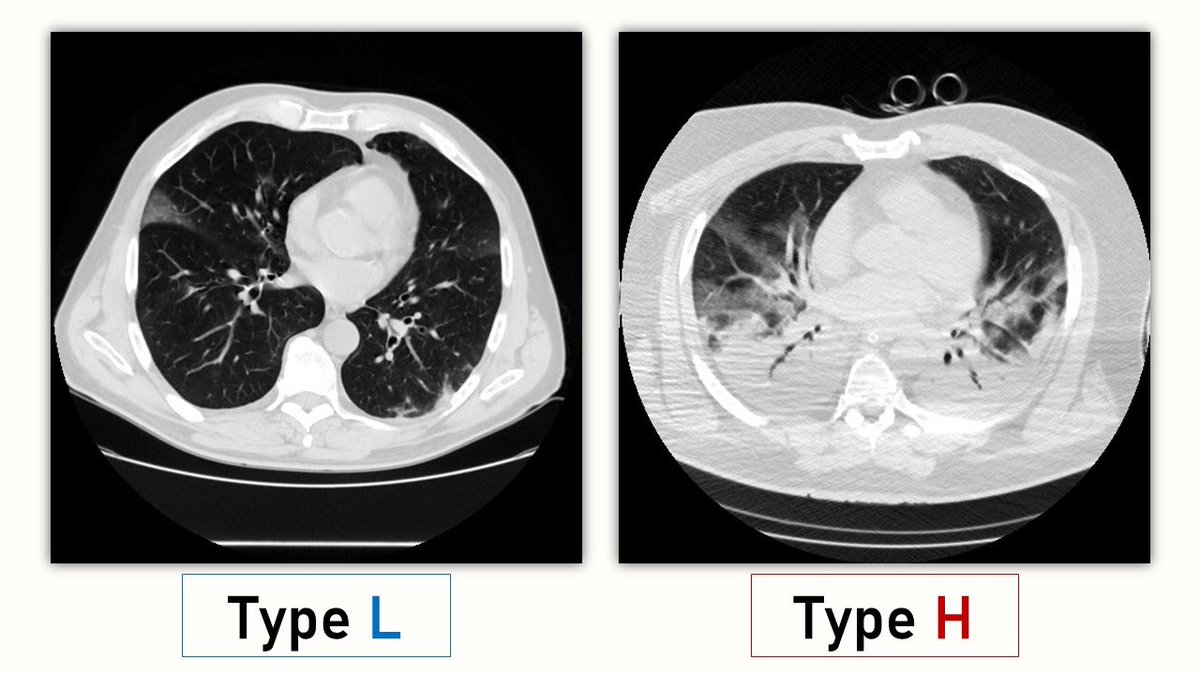
Gattinoni et al describe 2 phenotypes in #COVID2019 respiratory failure
Type L /Type H
Type L : early, normal compliance, low V:Q.
Type H : high elastance & high right to left shunt
For type L caution using high PEEP
#covidclinicalpearls /26
Type L /Type H
Type L : early, normal compliance, low V:Q.
Type H : high elastance & high right to left shunt
For type L caution using high PEEP
#covidclinicalpearls /26
#renal failure in #Covid_19 is fortunately rare 1-5% of all hospitalized patients
RRT needed in 5-20% of ICU cases
100% mortality in patients needing RRT in one large series
Reports of frequent clotting of circuit in CVVHD- use LMWH eary #covid19
#covidclinicalpearls /27
RRT needed in 5-20% of ICU cases
100% mortality in patients needing RRT in one large series
Reports of frequent clotting of circuit in CVVHD- use LMWH eary #covid19
#covidclinicalpearls /27
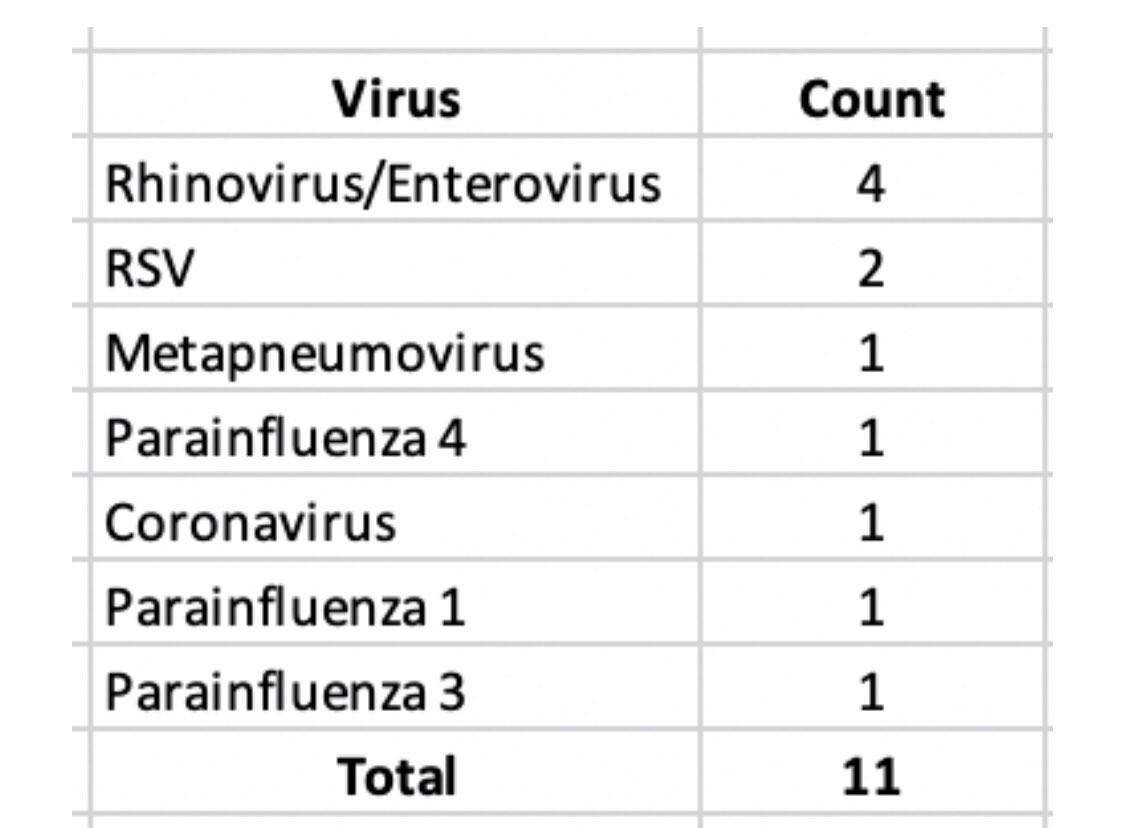
Co-infection rates can be high with #COVID19
Stanford group reports 22% coinfection rates with other viral infections in 49 #Covid_19 patients
#covidclinicalpearls /28
Stanford group reports 22% coinfection rates with other viral infections in 49 #Covid_19 patients
#covidclinicalpearls /28
Bacterial superinfection in #COVID19 rates are low 10-20%
#MRSA is typically not seen as with #influenza
#Azithromycin use with #Hydroxycloroquine has been shown to be effective ...
#covidclinicalpearls /29
#MRSA is typically not seen as with #influenza
#Azithromycin use with #Hydroxycloroquine has been shown to be effective ...
#covidclinicalpearls /29
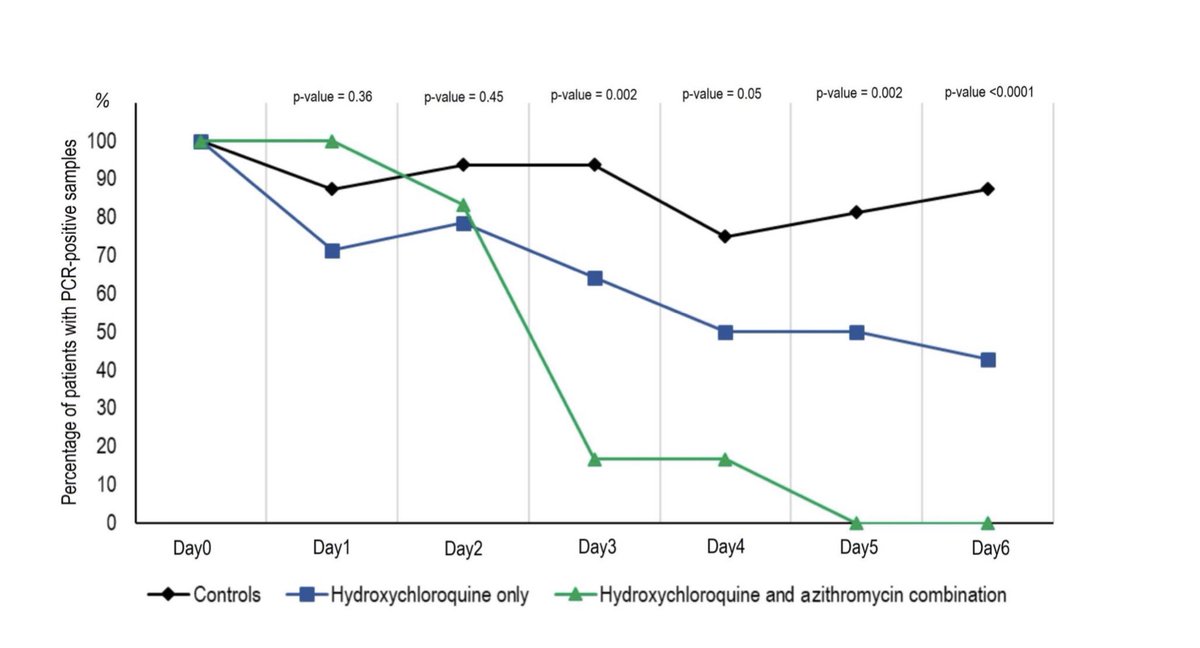
Use of #hydroxychloriquine and #Azithromycin was studied in 20 patients with #Covid_19 - showed significant reduction in viral carriage on Day6 vs controls
Evidence favoring use of #Azithromycin gaining
Caution due to QTc interval
#covidclinicalpearls /30
Evidence favoring use of #Azithromycin gaining
Caution due to QTc interval
#covidclinicalpearls /30
Criticism for Gautret et al #hydroxycholoroquine trial for #COVID19
Viral load higher in control group
AND
6 patients in HCQ group were excluded from analysis - 5 would have been considered #Covid_19 failures
Thus NO clear evidence for Azithro
#covidclinicalpearls /31
Viral load higher in control group
AND
6 patients in HCQ group were excluded from analysis - 5 would have been considered #Covid_19 failures
Thus NO clear evidence for Azithro
#covidclinicalpearls /31
UPenn protocol
#Hydroxychoroquine use is NOT recommended in
non-hospitalized patients and
hospitalized with mild disease
and
no risk factors
#Covid_19
#covidclinicalpearls /32
#Hydroxychoroquine use is NOT recommended in
non-hospitalized patients and
hospitalized with mild disease
and
no risk factors
#Covid_19
#covidclinicalpearls /32
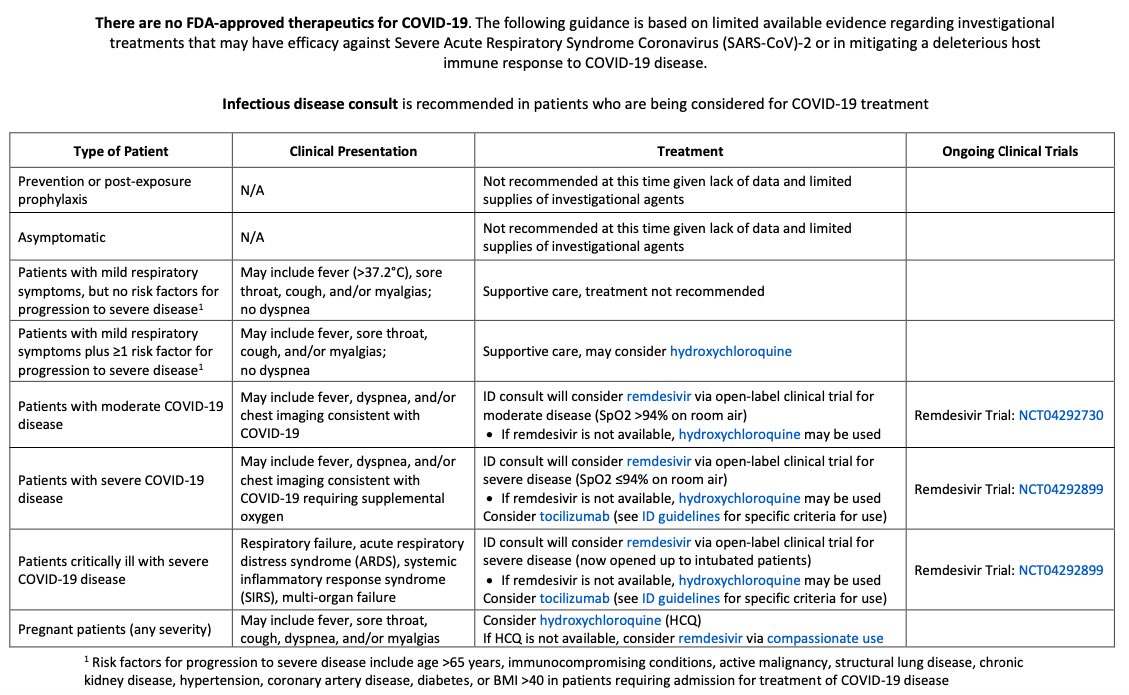
#antiviral use in #Covid_19
#Remdesevir is the only agent with universal consensus
This is algorithm at Brigham & Women’s
#covidclinicalpearls /33
#Remdesevir is the only agent with universal consensus
This is algorithm at Brigham & Women’s
#covidclinicalpearls /33
#Antiviral #Covid_19
#Lopinavir #Ritonavir combo could be useful
Cao et al (NEJM) considered a negative study
However trial DID show
▪️28 day mortality was lower
▪️~50% Shorter ICU Stay (6 vs 11 days)
Randomized only on D13 so likely too late
#covidclinicalpearls /34
#Lopinavir #Ritonavir combo could be useful
Cao et al (NEJM) considered a negative study
However trial DID show
▪️28 day mortality was lower
▪️~50% Shorter ICU Stay (6 vs 11 days)
Randomized only on D13 so likely too late
#covidclinicalpearls /34
#Antiviral #Covid_19
#Triple-therapy with
#Remdesivir
#Ritonavir
#Lopinavir
+ #interferon
+ #Hydroxychloroquine
🔹Is in clinical trials
🔹 Can be tried in center where available in moderate /severe disease or high risk #COVID19 patients
#covidclinicalpearls /35
#Triple-therapy with
#Remdesivir
#Ritonavir
#Lopinavir
+ #interferon
+ #Hydroxychloroquine
🔹Is in clinical trials
🔹 Can be tried in center where available in moderate /severe disease or high risk #COVID19 patients
#covidclinicalpearls /35
#Covid_19 IV Ig described in one case series by Cao. 5days 25g/d in 3 severe pts. More data needed
#chestpulmonary
#covidclinicalpearls /37
#chestpulmonary
#covidclinicalpearls /37
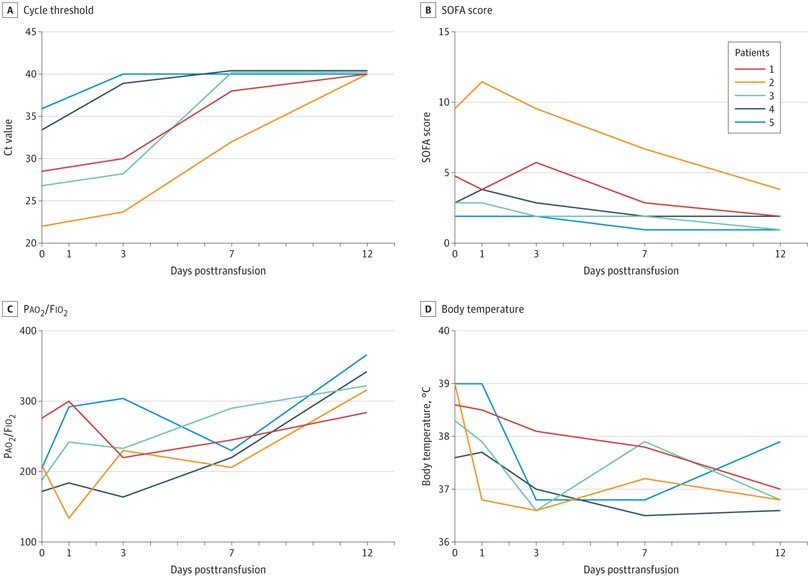
Convalescent plasma in #Covid_19 #ARDS
Donors
🔹asymptomatic x10d
🔹Ab titer >1:1000(Elisa) & >1:40 (neutral)
ALL 5 recovered
This is the most promising #treatment for #COVID19
All hospitals must initiate protocols for plasma pheresis from survivors
#covidclinicalpearls /38
Donors
🔹asymptomatic x10d
🔹Ab titer >1:1000(Elisa) & >1:40 (neutral)
ALL 5 recovered
This is the most promising #treatment for #COVID19
All hospitals must initiate protocols for plasma pheresis from survivors
#covidclinicalpearls /38
A new study now casts doubt on efficacy of #Hydroxychloroquine and #Azithromycin
80% of patients in this study had no viral clearance on D5-6 after therapy
#covidclinicalpearls /39
pdf.sciencedirectassets.com/272288/AIP/1-s…
80% of patients in this study had no viral clearance on D5-6 after therapy
#covidclinicalpearls /39
pdf.sciencedirectassets.com/272288/AIP/1-s…
I don’t know who needs to hear this
#Covid_19 #pneumonia #ARDS is NOT #HAPE ; nor similar to it.
#covidclinicalpearls /40
#Covid_19 #pneumonia #ARDS is NOT #HAPE ; nor similar to it.
#covidclinicalpearls /40
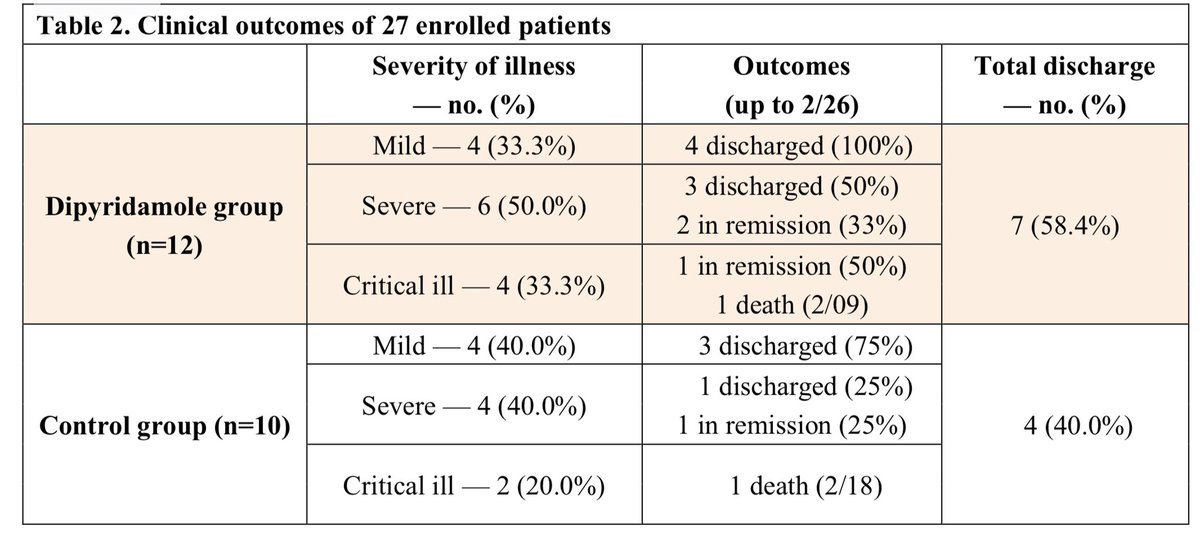
Extensive Intravascular microthrombosis is seen in autopsy in #Covid_19
#Dipyridamole has been shown to decrease D Dimer levels and clinical benefit in 1 study
#covidclinicalpearls /41
#Dipyridamole has been shown to decrease D Dimer levels and clinical benefit in 1 study
#covidclinicalpearls /41
#tocilizumab is being tried in critically ill patients with #covid_19
15 patients with severe #covid19 & ⬆️ #IL6 levels (2X - 90X normal)
10 of 15 improved
3 of 4 that received only single dose died
onlinelibrary.wiley.com/doi/epdf/10.10…
#covidclinicalpearls /42
15 patients with severe #covid19 & ⬆️ #IL6 levels (2X - 90X normal)
10 of 15 improved
3 of 4 that received only single dose died
onlinelibrary.wiley.com/doi/epdf/10.10…
#covidclinicalpearls /42
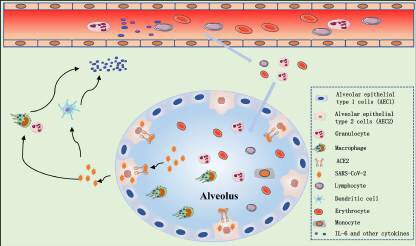
#SARSCoV2 infects AEC2 thru ACE2 receptor➡️destruction of epithelial cells ➡️release of virus➡️activate the innate immune system➡️release ⏫cytokines incl #IL6 Adaptive immunity also activated by dendritic cells
#Covid_19 molecular pathogenesis & #IL6
#covidclinicalpearls /42
#Covid_19 molecular pathogenesis & #IL6
#covidclinicalpearls /42
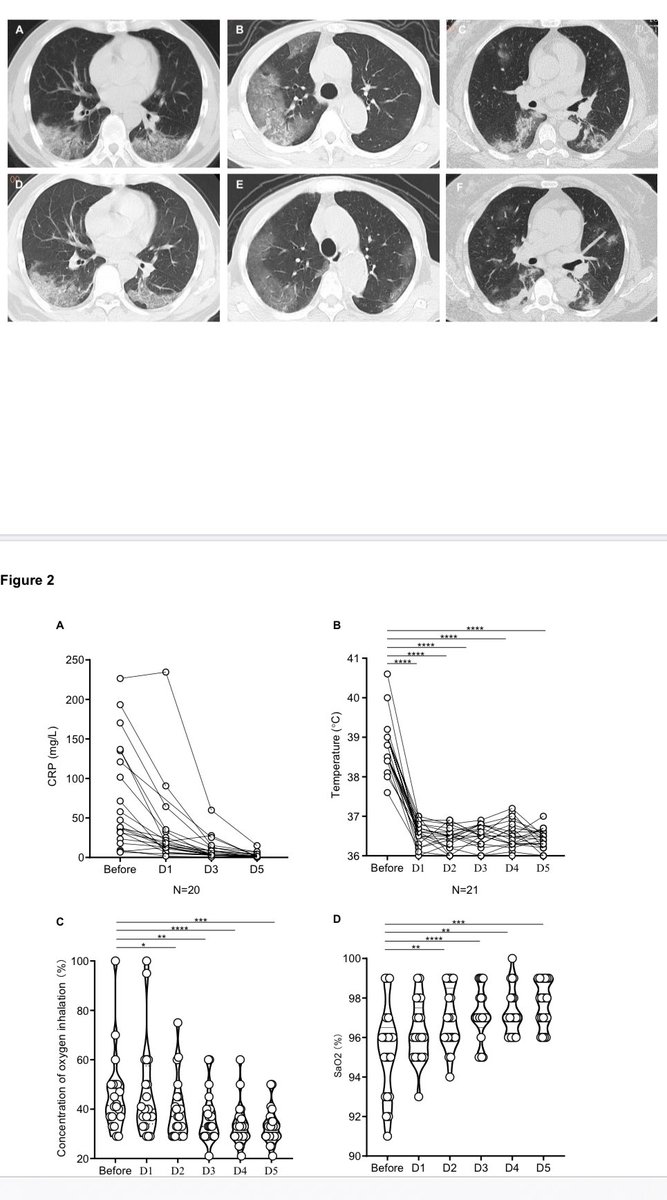
#Tocilizumab in #COVID19
21 #Covid_19 patients 17 severe & 4 critical
All patients improved -19 discharged ~ avg D13
75% ⬇️ lowered FiO2 levels
CT improvement in 90%
#covidclinicalpearls /43
21 #Covid_19 patients 17 severe & 4 critical
All patients improved -19 discharged ~ avg D13
75% ⬇️ lowered FiO2 levels
CT improvement in 90%
#covidclinicalpearls /43
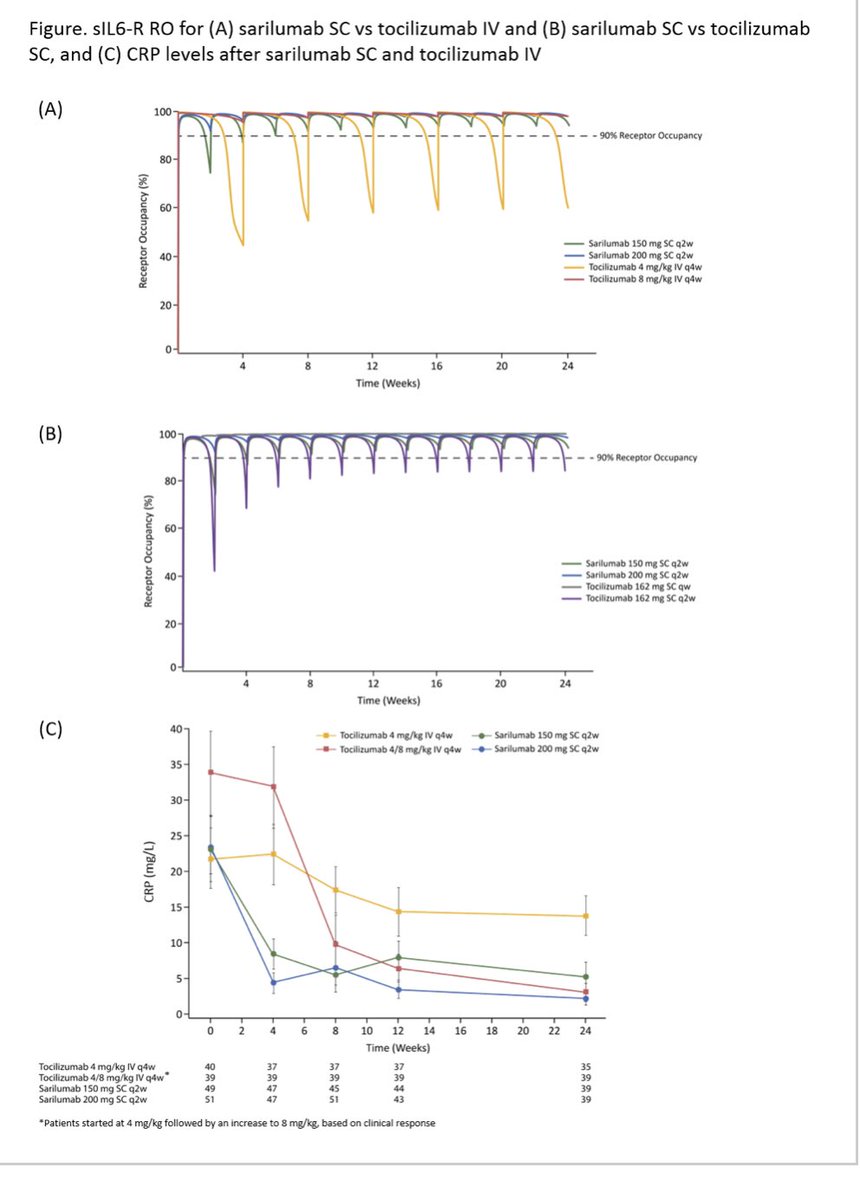
A clinical trial for #sarilumab another #IL6 blocker in #Covid_19 is currently underway;
Attractive alternative to #Tocilizumab for #COVID19
#Sarilumab higher #IL6 R binding affinity vs #Tocilizumab
#covidclinicalpearls /44
Attractive alternative to #Tocilizumab for #COVID19
#Sarilumab higher #IL6 R binding affinity vs #Tocilizumab
#covidclinicalpearls /44
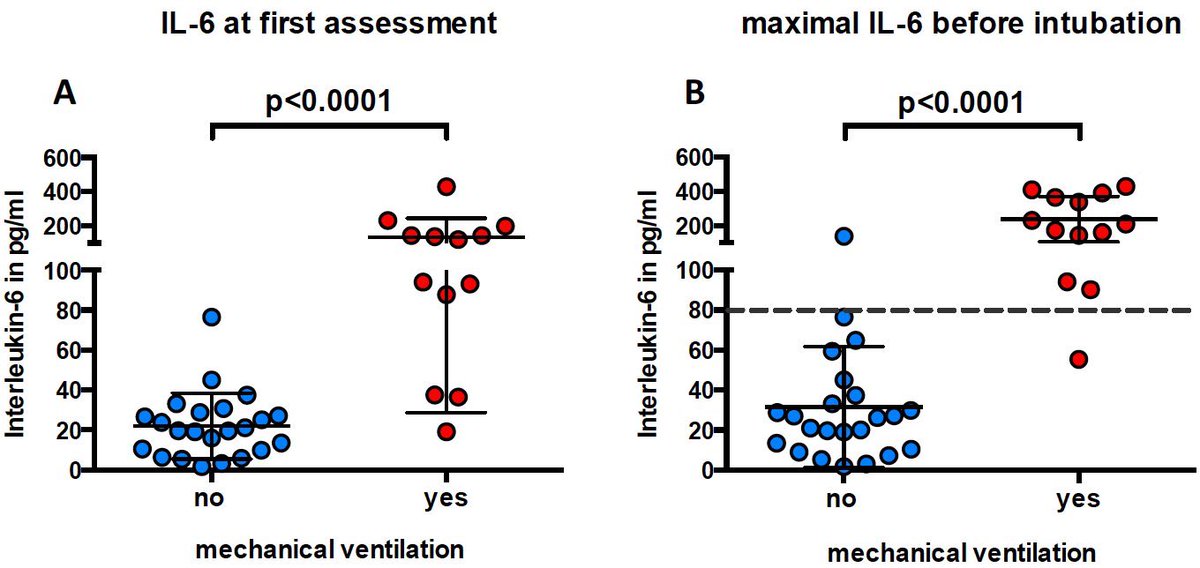
Maximal #IL6 highly predictive of respiratory failure in #COVIDー19
For #IL6 ≥ 80pg/ml, risk of respiratory failure was 92%
Sound rationale for #Tocilizumab #sarilumab in #COVID19
#covidclinicalpearls / 45
For #IL6 ≥ 80pg/ml, risk of respiratory failure was 92%
Sound rationale for #Tocilizumab #sarilumab in #COVID19
#covidclinicalpearls / 45
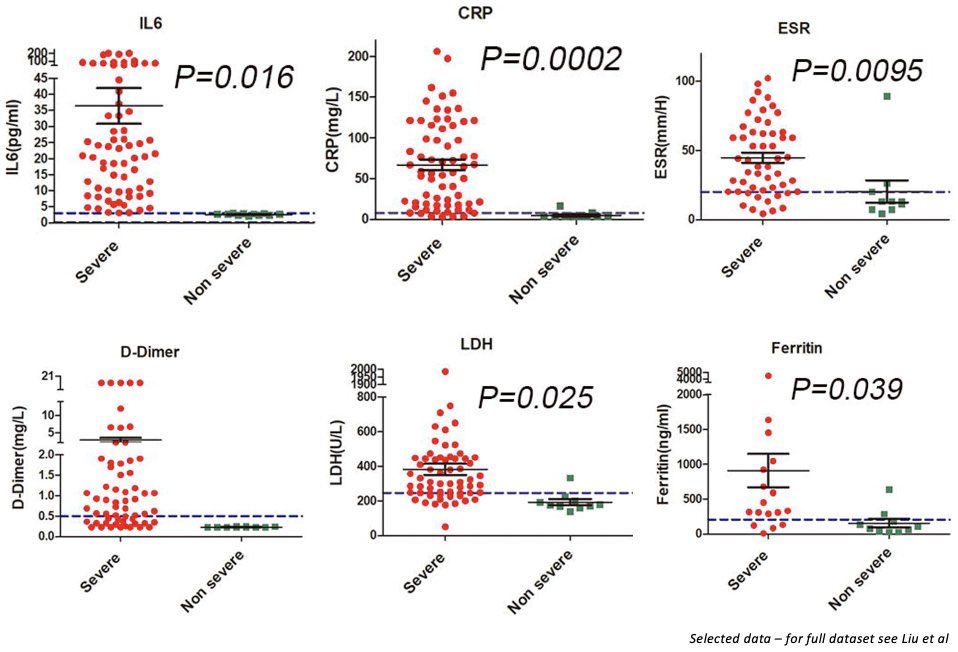
Patients at risk for #CytokineStorm in #COVIDー19 should be identified with serum biomarkers
#DDimer
#Ferritin
#LDH
#IL6
If ⬆️ start #Tocilizumab early + #steroids + #anticoag (for ⬆️DDimer)
#covidclinicalpearls / 46
#DDimer
#Ferritin
#LDH
#IL6
If ⬆️ start #Tocilizumab early + #steroids + #anticoag (for ⬆️DDimer)
#covidclinicalpearls / 46

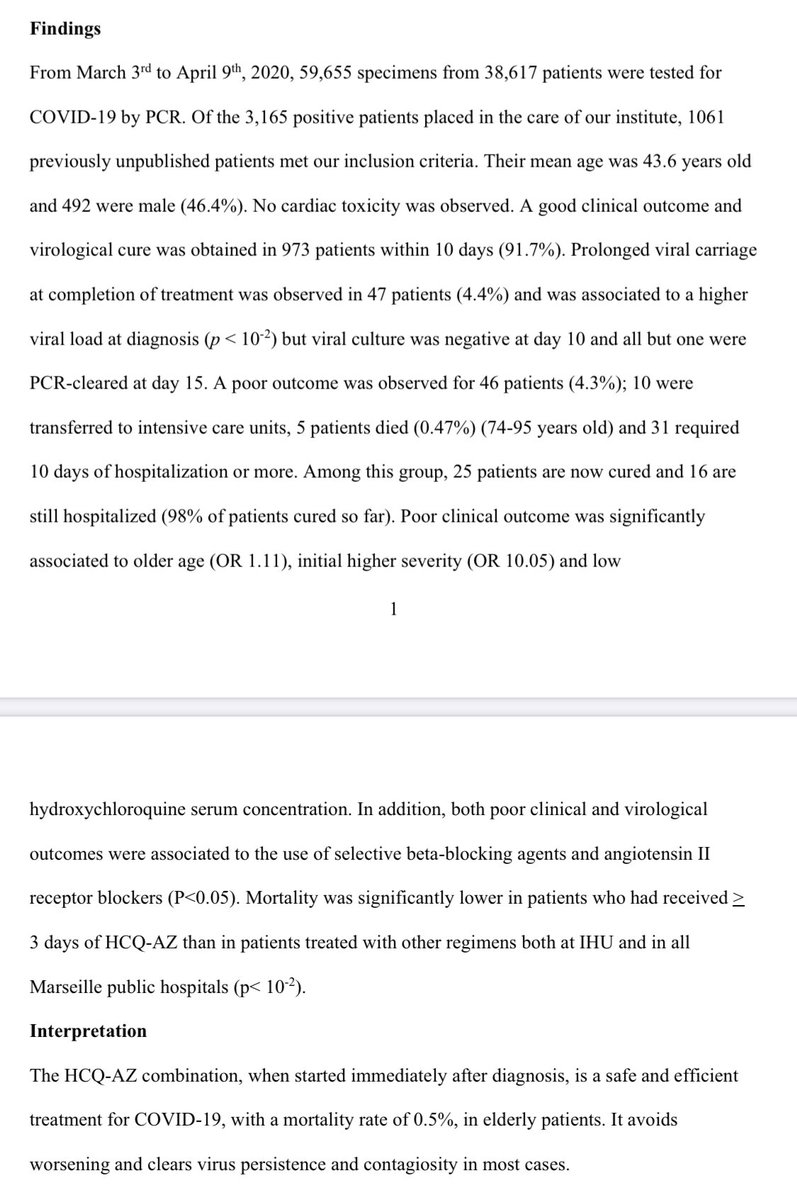
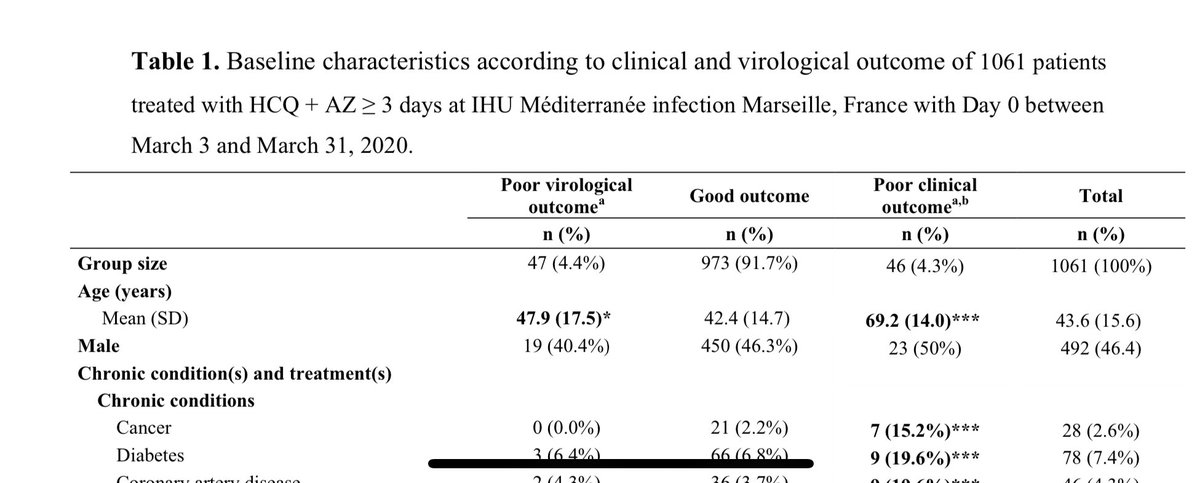
#Hydroxychloroquine and #Azithromycin combinations in #Covid_19 - more data from France - this is likely the 3rd study (pre-publication) Raoult et al
▫️91.7% positive clinical outcome & virologic cure
▫️NO cardiac toxicity
▫️1061 patients; 5 deaths
#covidclinicalpearls /48
▫️91.7% positive clinical outcome & virologic cure
▫️NO cardiac toxicity
▫️1061 patients; 5 deaths
#covidclinicalpearls /48
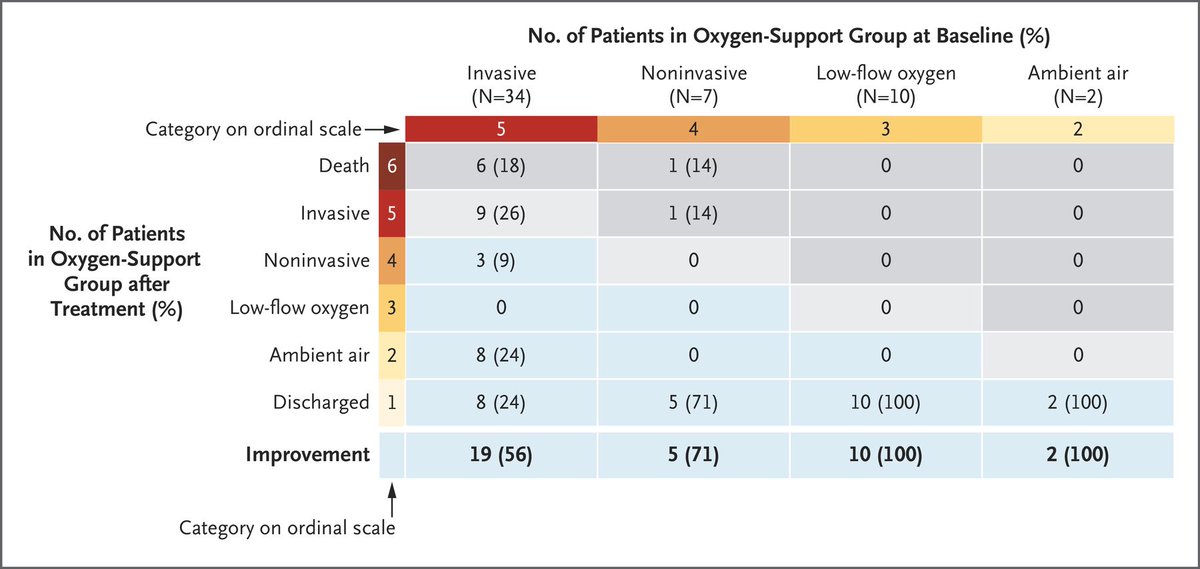
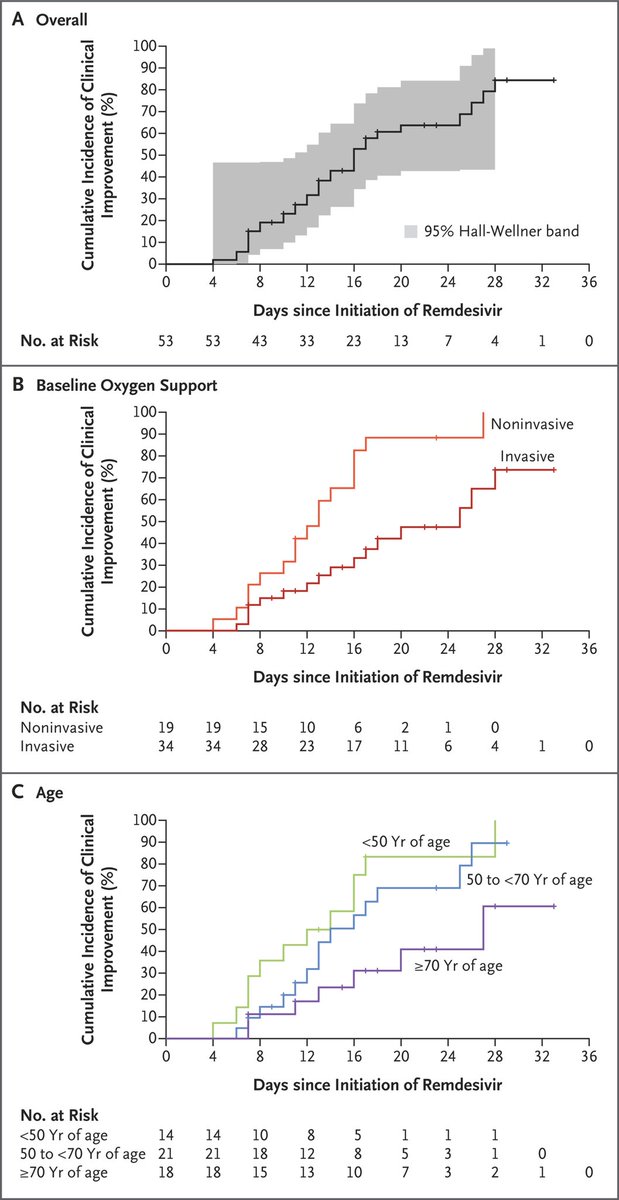
#remdesevir in #COVIDー19 respiratory failure
53 patients
17/30 (57%) on vent extubated,
3/4 on ECMO weaned off
Overall 13% mortality
Mortality for those on vent 18% (much lower than historic controls)
Not a RCT but excellent results #covid19
#covidclinicalpearls /49
53 patients
17/30 (57%) on vent extubated,
3/4 on ECMO weaned off
Overall 13% mortality
Mortality for those on vent 18% (much lower than historic controls)
Not a RCT but excellent results #covid19
#covidclinicalpearls /49
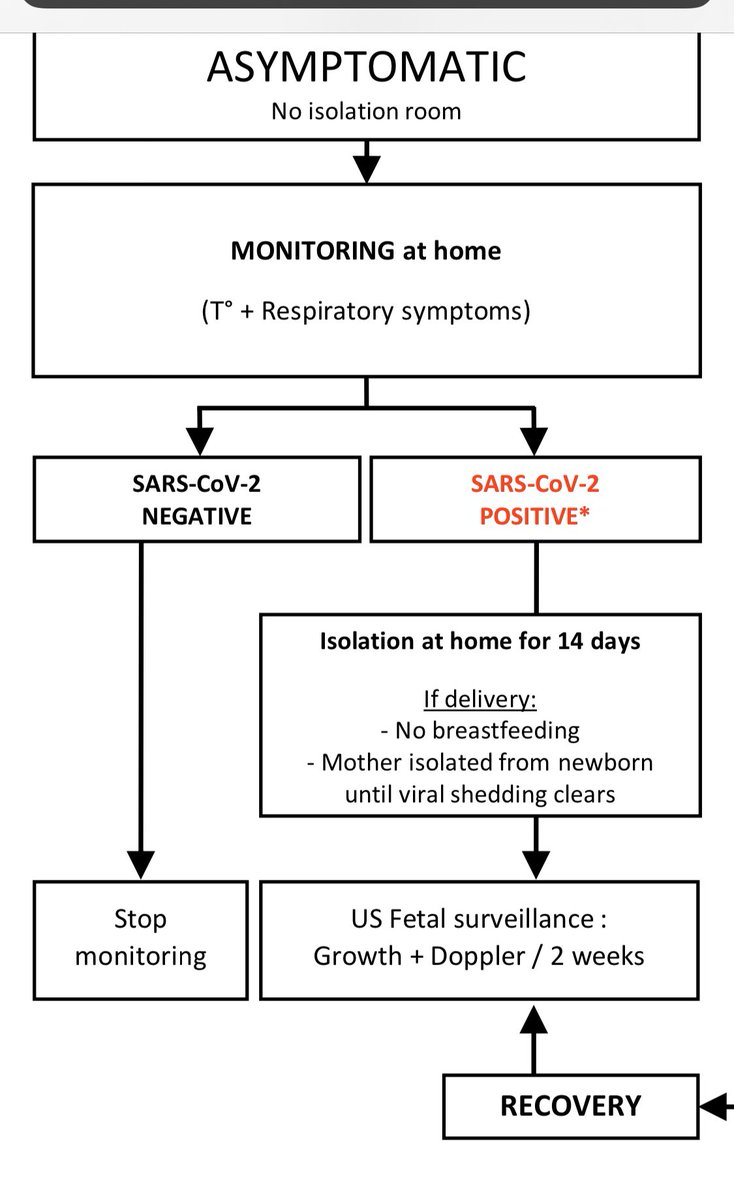
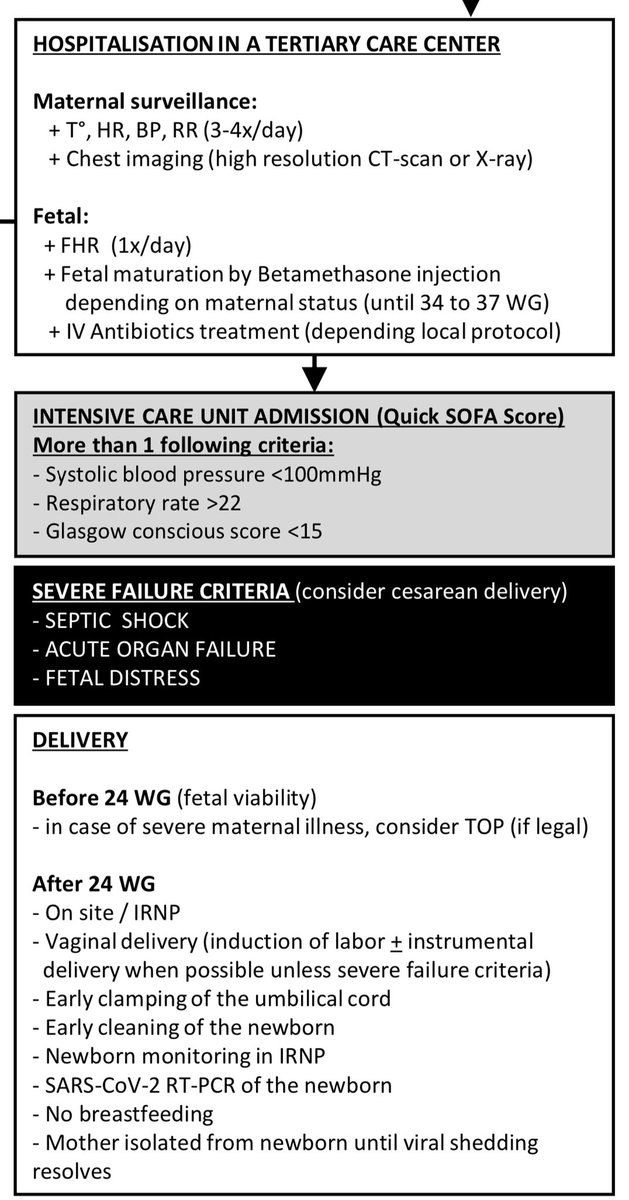
#pregnancy in #COVID19
Spanish algorithm
Mild #COVID__19 illness - bimonthly fetal growth ultrasounds and Doppler.
Vaginal delivery via induction of labour favoured to avoid unnecessary surgical complications unless septic shock/MSOF
#covidclinicalpearls /50
Spanish algorithm
Mild #COVID__19 illness - bimonthly fetal growth ultrasounds and Doppler.
Vaginal delivery via induction of labour favoured to avoid unnecessary surgical complications unless septic shock/MSOF
#covidclinicalpearls /50
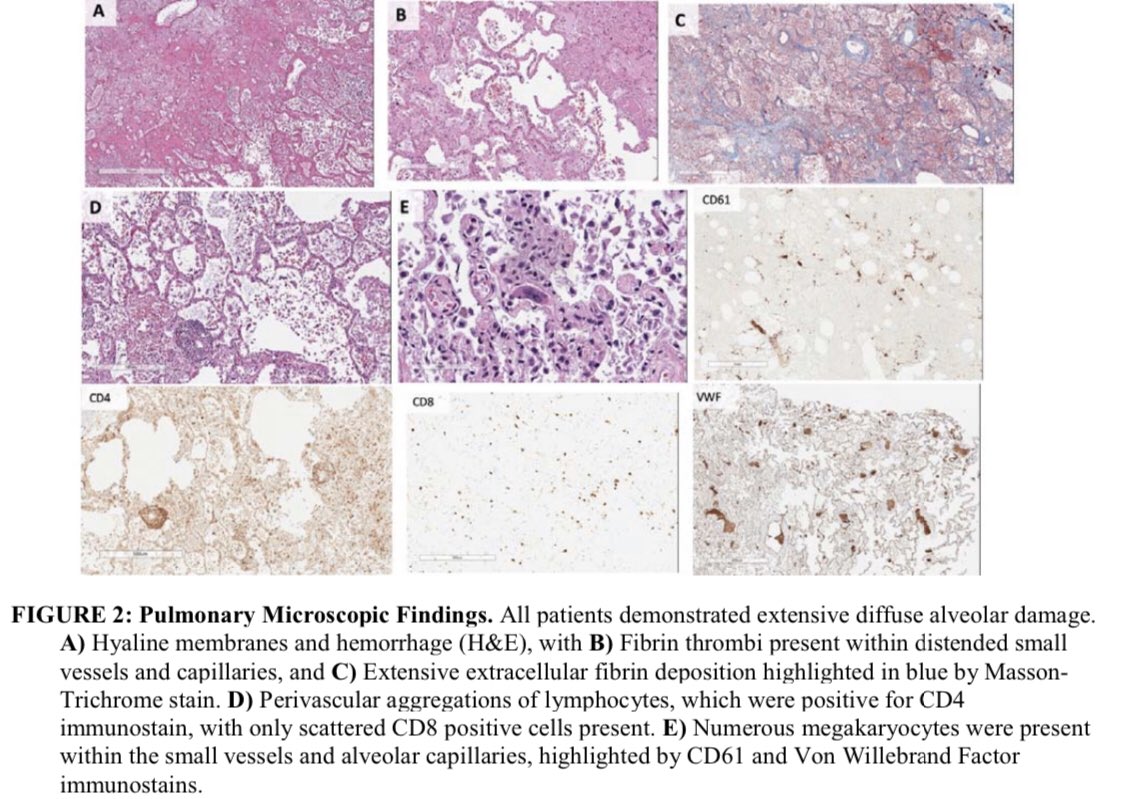
#Pathology in #COVID19 autopsy findings
Thrombotic microangiopathy restricted to the lungs.
Small vessel thrombus formation in the lung periphery in many cases with foci of alveolar hemorrhage.
No secondary infection
#Covid_19
#covidclinicalpearls /51
Thrombotic microangiopathy restricted to the lungs.
Small vessel thrombus formation in the lung periphery in many cases with foci of alveolar hemorrhage.
No secondary infection
#Covid_19
#covidclinicalpearls /51
#COVID__19 Lab markers provide important insight into prognosis & hence need to be monitored closely even in patients who appear stable.
#DDimer #ferritin #IL6 #lymphocyte % #LDH
#covid19
#covidclinicalpearls /52
#DDimer #ferritin #IL6 #lymphocyte % #LDH
#covid19
#covidclinicalpearls /52
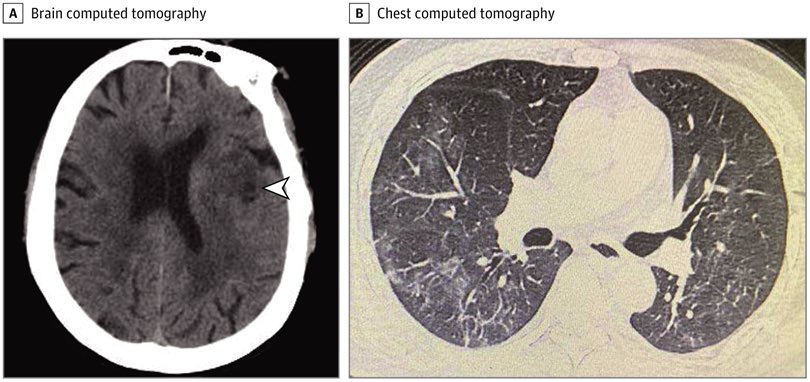
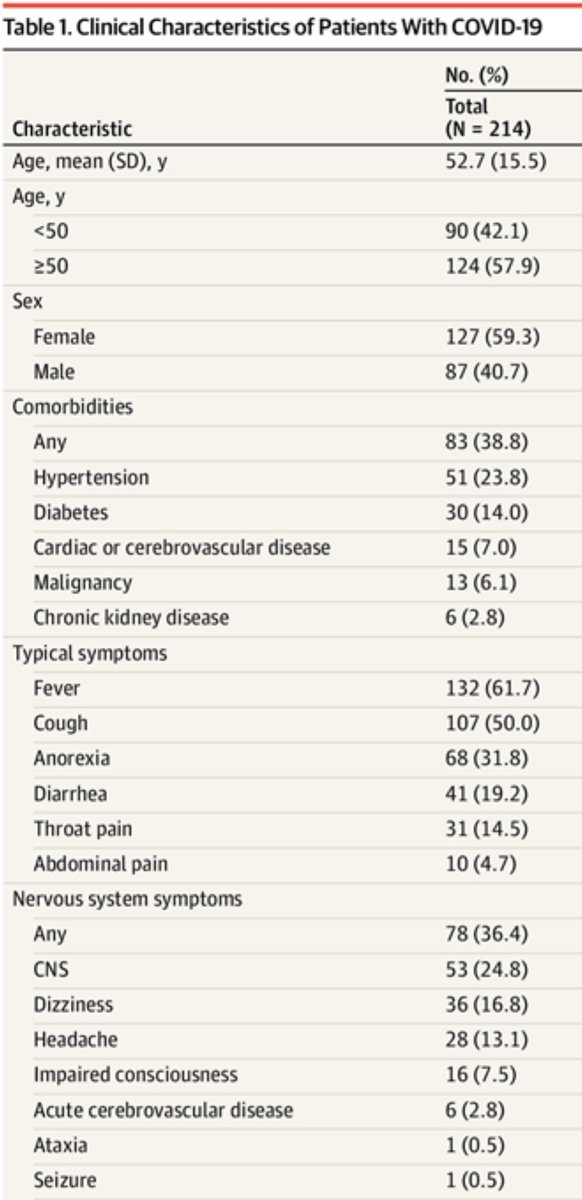
#COVID__19 CNS manifestations including #CVA #stroke are reported
Case series from #Wuhan describes 6 cases /214 presenting with ischemic stroke / hemiplegia & 16 with impaired LOC
Patients may not manifest typical symptoms of #covid19 infection
#covidclinicalpearls / 53
Case series from #Wuhan describes 6 cases /214 presenting with ischemic stroke / hemiplegia & 16 with impaired LOC
Patients may not manifest typical symptoms of #covid19 infection
#covidclinicalpearls / 53
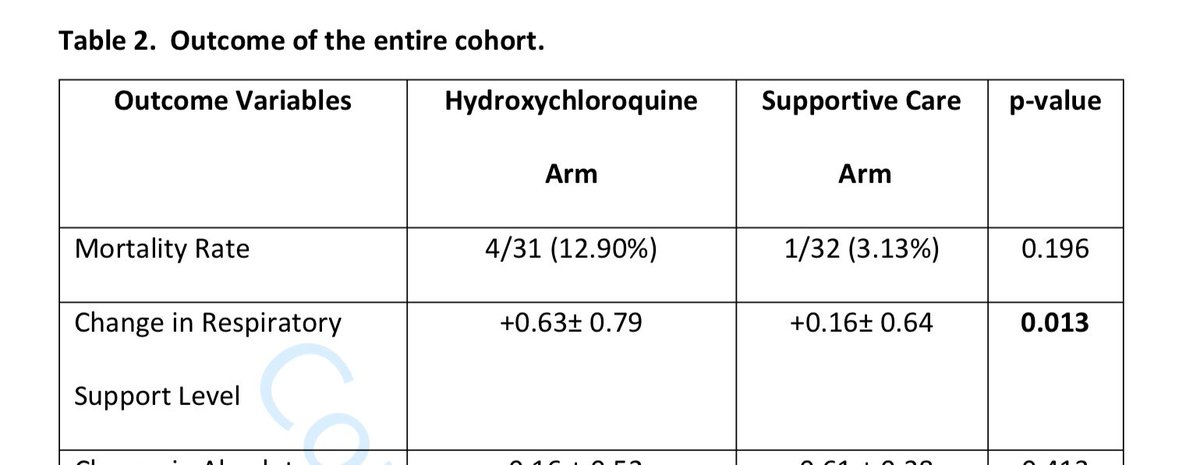
#Hydroxychloroquine in #covid19 story gets murkier everyday.
#HCQ vs supportive care compared in 63 #COVID__19 pts
#Hydroxychloroquine associated with a need for ⬆️respiratory support & ⬆️risk for intubation by D5
Mortality HCQ 4/31 (vs 1/32)
#covidclinicalpearls /54
#HCQ vs supportive care compared in 63 #COVID__19 pts
#Hydroxychloroquine associated with a need for ⬆️respiratory support & ⬆️risk for intubation by D5
Mortality HCQ 4/31 (vs 1/32)
#covidclinicalpearls /54

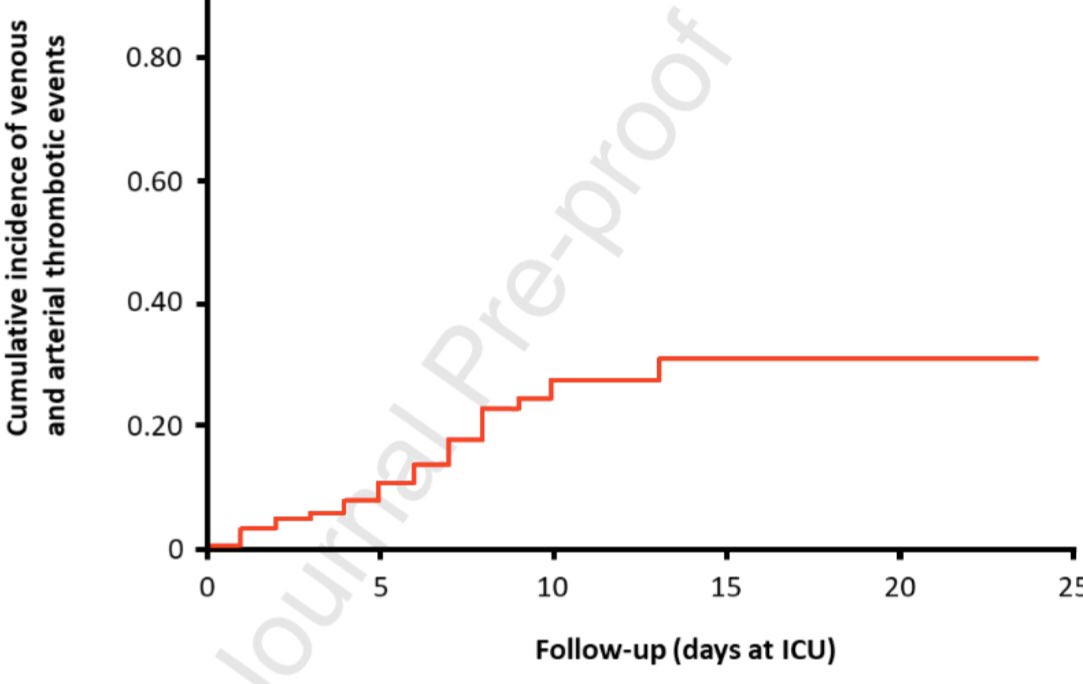
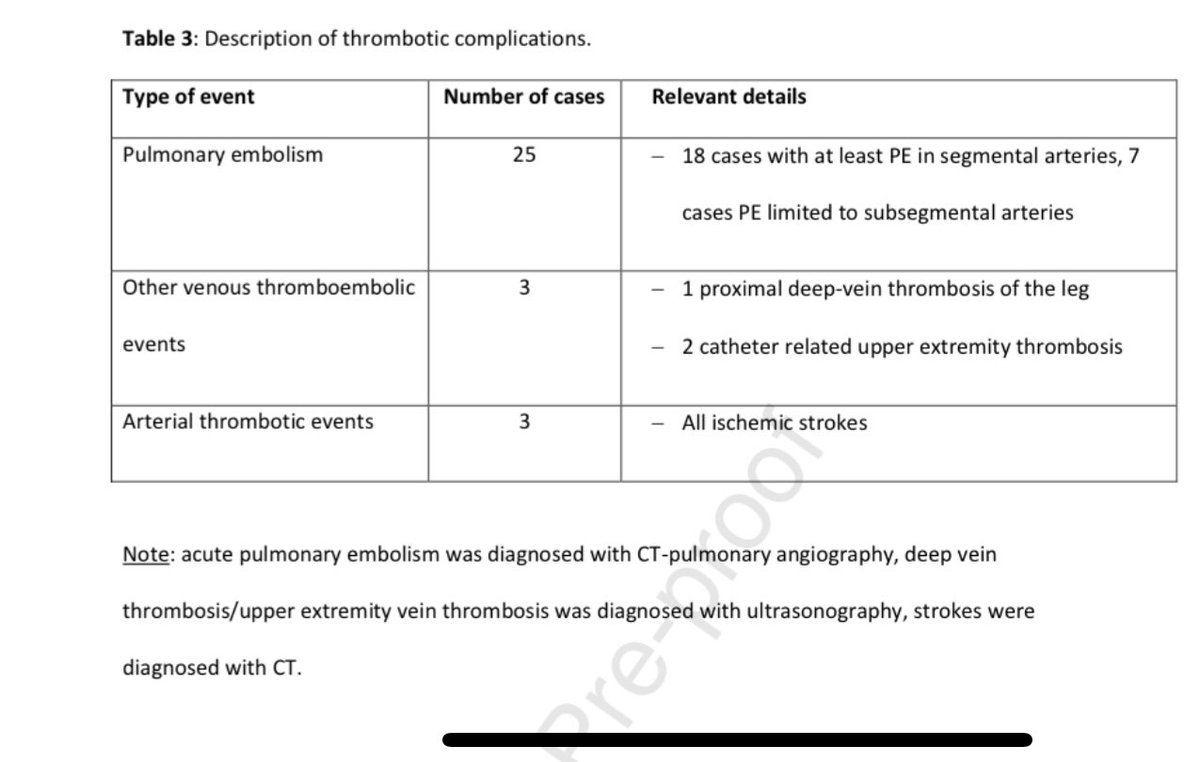
#COVID__19 High prevalence of thromboembolism even in patients receiving prophylaxis.
Dutch series 184 ICU #COVID19 patients
31% incidence of #thrombotic complication
#Pulmonaryembolism was the most frequent thrombotic complication (n=25)
#covidclinicalpearls /55
Dutch series 184 ICU #COVID19 patients
31% incidence of #thrombotic complication
#Pulmonaryembolism was the most frequent thrombotic complication (n=25)
#covidclinicalpearls /55
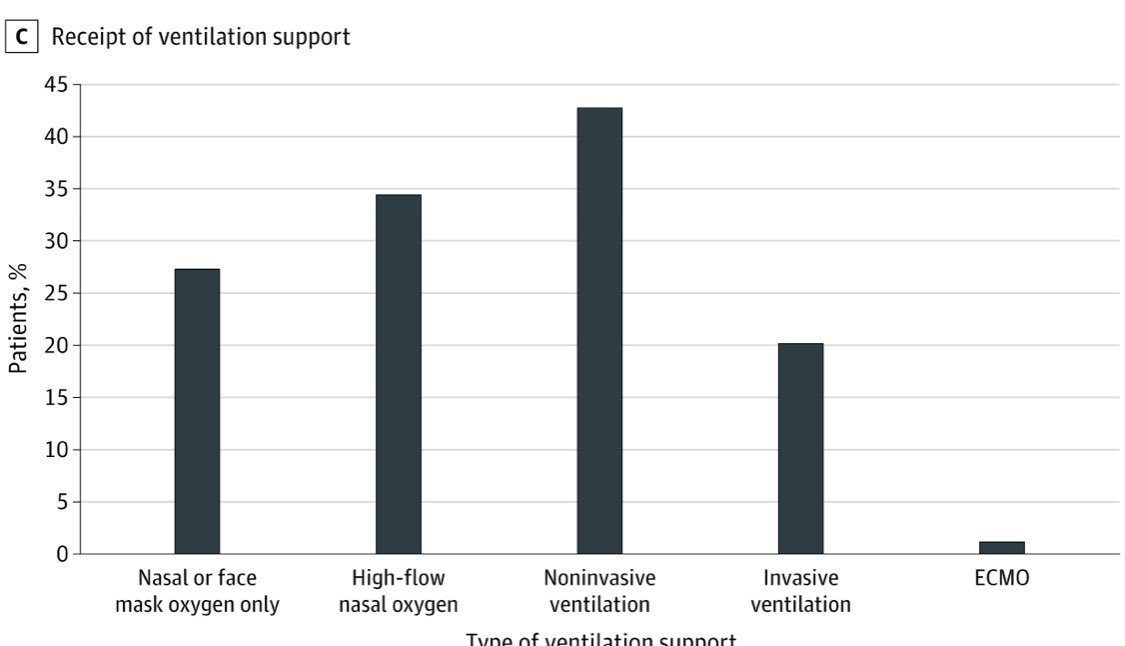
#COVID19 Just ~ 20% of patients who died in #Wuhan received mechanical #ventilation !
Partly related to shortage of vents (?)
Also underscores #COVID__19 patients can deteriorate quickly. Need to monitor closely & intervene early
#covidclinicalpearls / 56
Partly related to shortage of vents (?)
Also underscores #COVID__19 patients can deteriorate quickly. Need to monitor closely & intervene early
#covidclinicalpearls / 56
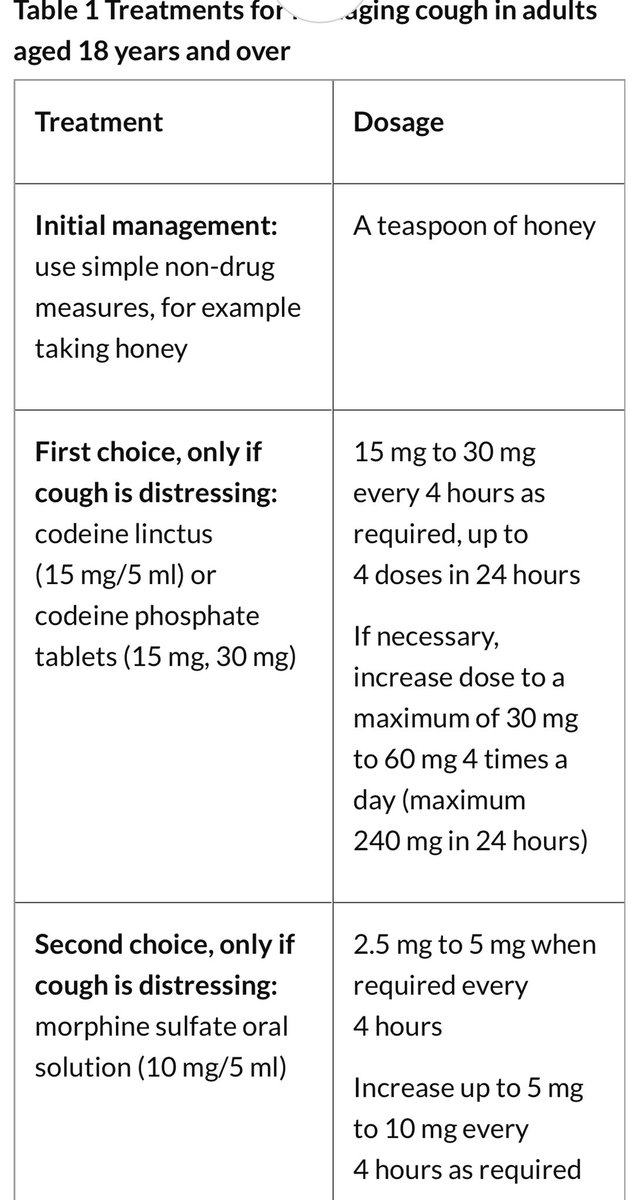
Cough in patients with #COVID__19 tends to be especially severe & often resistant to standard #antitussive measures.
#Morphine 2.5 - 5mg q4 suggested in these #COVID19 patients.
#covidclinicalpearls / 57
#Morphine 2.5 - 5mg q4 suggested in these #COVID19 patients.
#covidclinicalpearls / 57
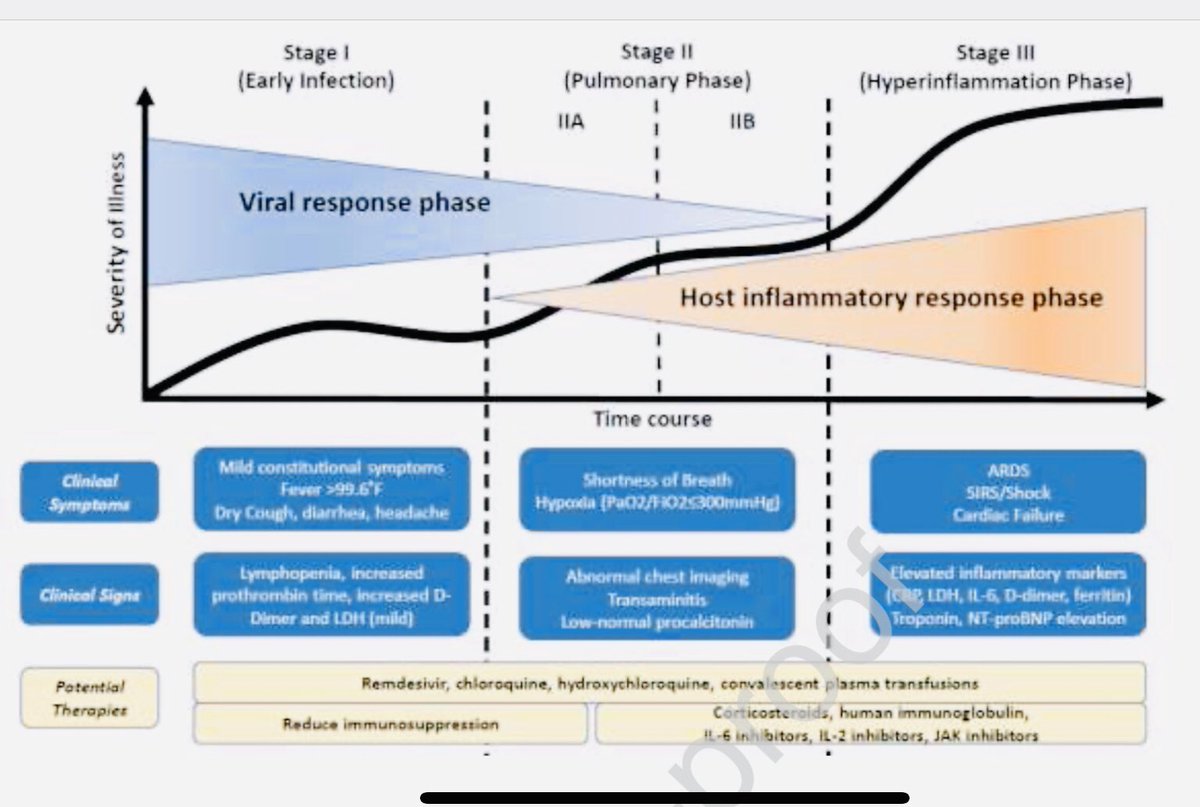
#COVID19
3 phase model of pathogenesis
Stg1 : early infection
#Antiviral
Stg 2 Pulm involvement 2A without & 2B with hypoxia
#Steroid use in 2B
Stg 3 #CytokineStorm & systemic #HLH
#Steroid #Tocilizumab
#covidclinicalpearls / 58
3 phase model of pathogenesis
Stg1 : early infection
#Antiviral
Stg 2 Pulm involvement 2A without & 2B with hypoxia
#Steroid use in 2B
Stg 3 #CytokineStorm & systemic #HLH
#Steroid #Tocilizumab
#covidclinicalpearls / 58
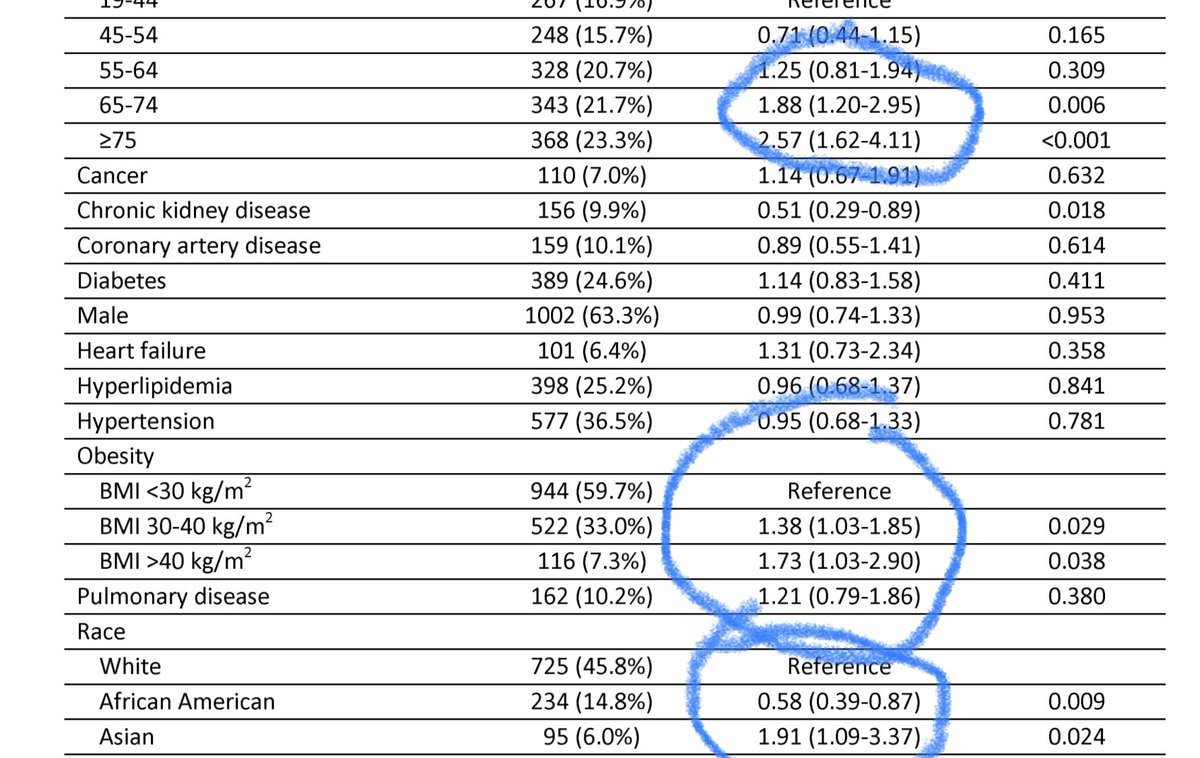
Biggest risk factors associated with severity of #COVID19 pneumonia are Age > 70; Adiposity #Obesity BMI > 40 & #Asian ethnicity
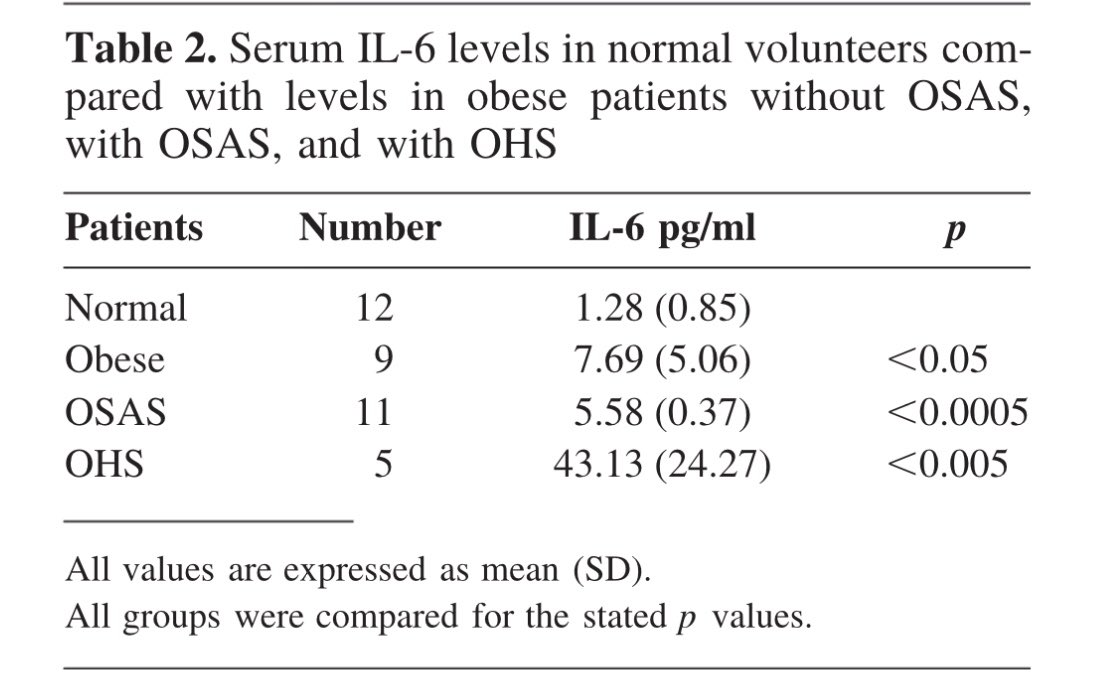
Obesity & OSA are associated with ⬆️ #IL6 levels & may be ➡️exaggerated #CytokineStorm in #COVID__19
#covidclinicalpearls /59
Obesity & OSA are associated with ⬆️ #IL6 levels & may be ➡️exaggerated #CytokineStorm in #COVID__19
#covidclinicalpearls /59
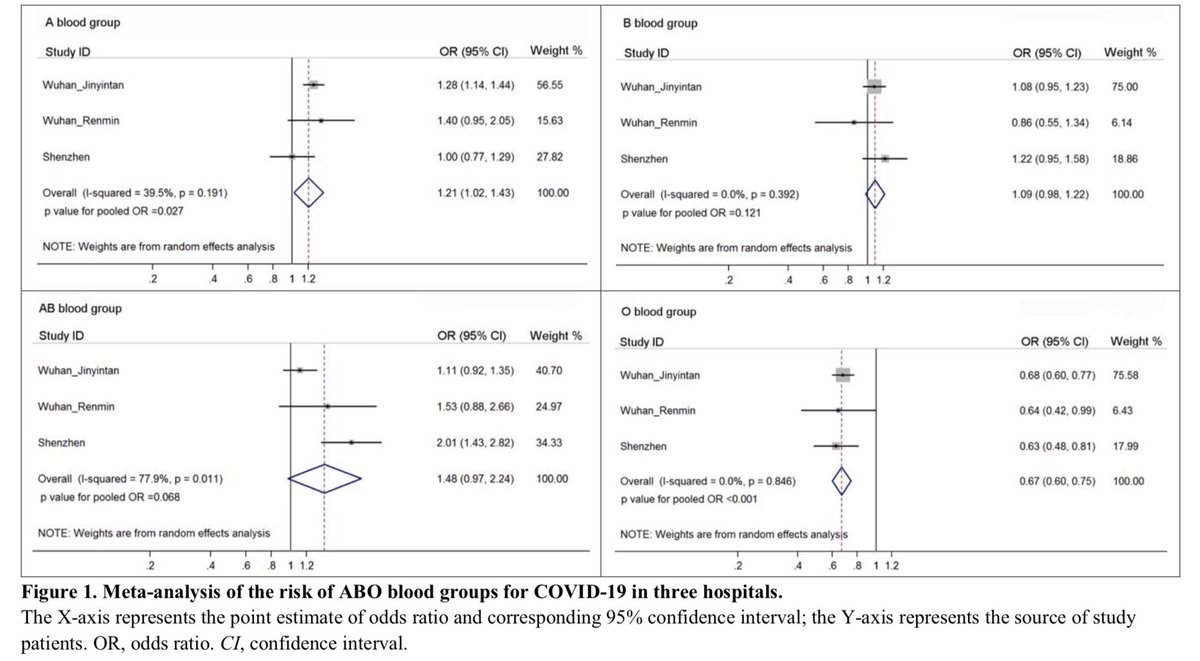
#Bloodgroup analysis of #COVID19 from China appear to show
A predilection for #blood group A (38% cases; OR 1.28)
&
A relative protection with blood group O (25% of cases; OR 0.68)
Similar distribution seen with #SARS previously
#covidclinicalpearls / 60
A predilection for #blood group A (38% cases; OR 1.28)
&
A relative protection with blood group O (25% of cases; OR 0.68)
Similar distribution seen with #SARS previously
#covidclinicalpearls / 60

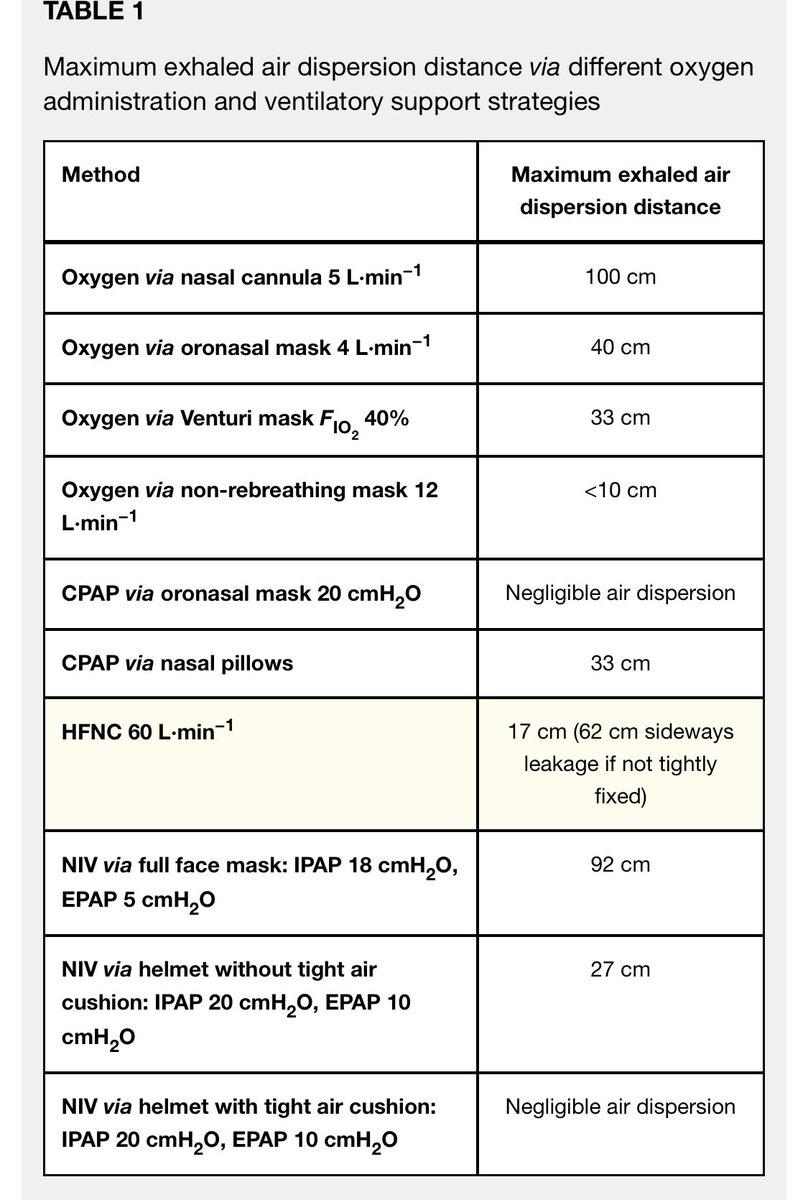
Protecting #HealthWorkers in #COVID19 rooms includes using #oxygen including #highflow and #NIV in ways that minimize aerosol dispersion & potential infection.
#O2 via NRB better than nasal canula
#NPPV via helmet with air tight cushion works best
#covidclinicalpearls / 62
#O2 via NRB better than nasal canula
#NPPV via helmet with air tight cushion works best
#covidclinicalpearls / 62
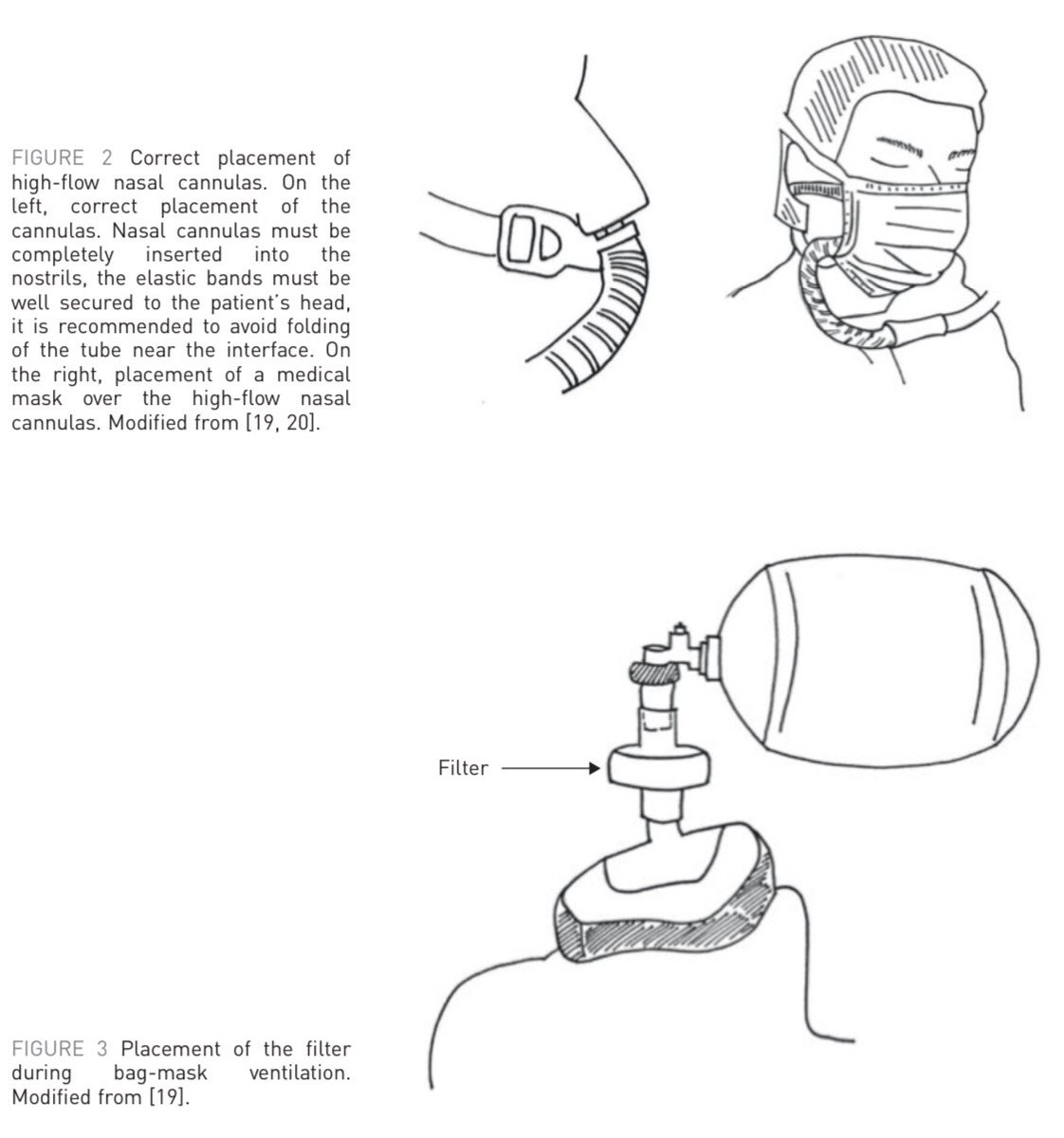
Correct placement of high flow oxygen nasal canula #HFNC & bag mask ventilation in patients with #COVID19
Important to prevent aerosol dispersion & protect #HealthWorkers in #Covid_19
#covidclinicalpearls / 63
Important to prevent aerosol dispersion & protect #HealthWorkers in #Covid_19
#covidclinicalpearls / 63
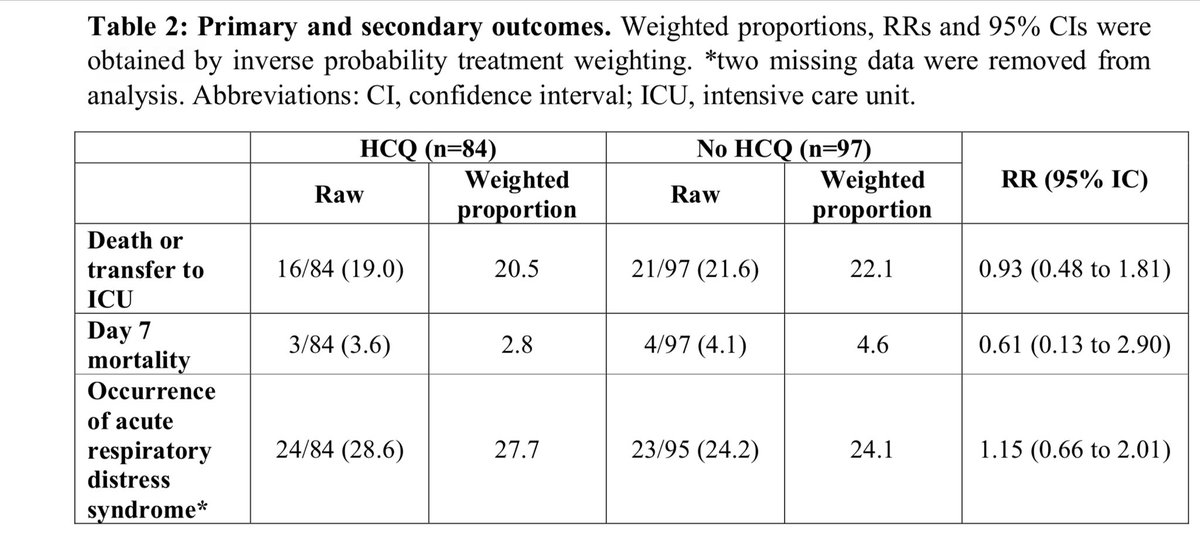
Yet another #Fail #Hydroxycloroquine study in #COVID19 also from France from 4 centers
NO difference in ICU admission, ARDS or Mortality in #covid_19
medrxiv.org/content/10.110…
#covidclinicalpearls / 64
NO difference in ICU admission, ARDS or Mortality in #covid_19
medrxiv.org/content/10.110…
#covidclinicalpearls / 64
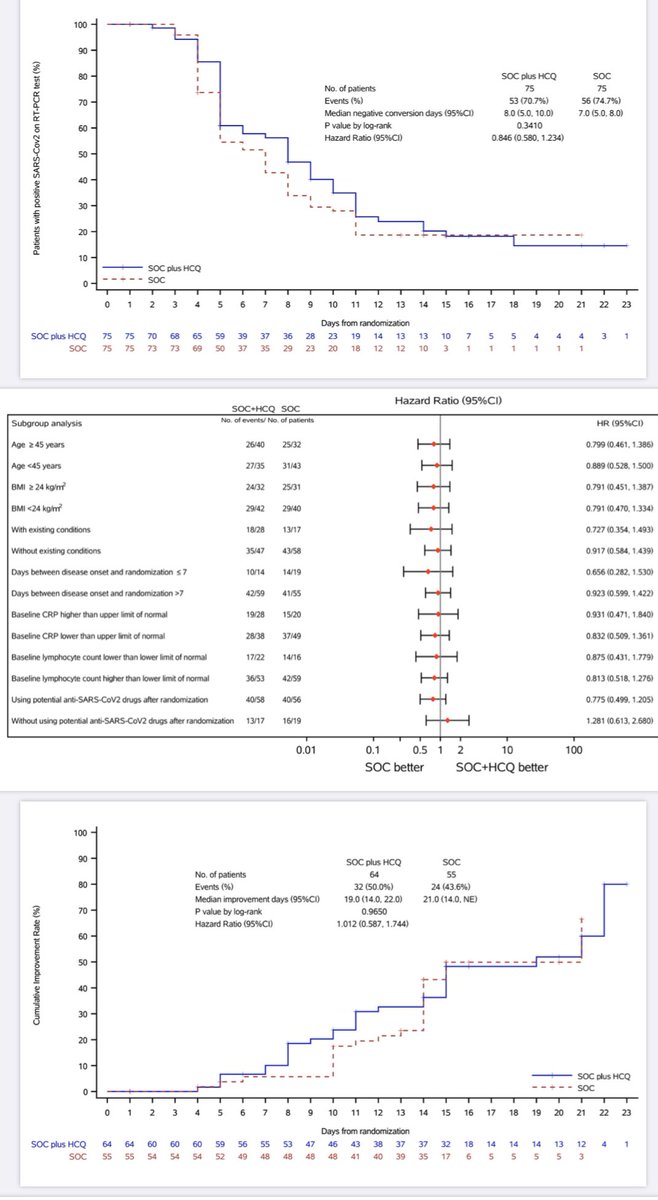
#Hydroxychloroquine in #COVID19 another #FAIL
150 hospitalized #Covid_19 RCT - #HCQ vs SOC
Day28 viral negative conversion rate was not different 85.4% vs 81.3%.
No difference in symptoms alleviation rate D28
30% adverse events in HCQ; 2 SAE.
#covidclinicalpearls / 65
150 hospitalized #Covid_19 RCT - #HCQ vs SOC
Day28 viral negative conversion rate was not different 85.4% vs 81.3%.
No difference in symptoms alleviation rate D28
30% adverse events in HCQ; 2 SAE.
#covidclinicalpearls / 65