THREAD: Yesterday, we saw negative narratives from my #TransHealthEthicsProject interviews with #trans folks re: #healthcare. Most had a mix of both pos & neg. What does good care look like? And what are some tips/guidelines for delivering it? 1/n
#TransAwarenessWeek #bioethics
#TransAwarenessWeek #bioethics
Let's start w/Simon, whose negative experiences we saw yesterday, including being misgendered and outed by front office staff, especially when he sought Gyn care. I asked all participants to say what would be better--or in fact was better sometimes--than negative experiences. 2/n
Simon said "I think better responses are just, if they’re asking if you’re a new patient starting with
basic things rather than starting with a birthdate, because that kind of breaks it down. It seems
weird but if you start with a birthdate then we can start somewhere..." 3/n
basic things rather than starting with a birthdate, because that kind of breaks it down. It seems
weird but if you start with a birthdate then we can start somewhere..." 3/n
"...it makes a difference [if] instead of saying 'what’s your name?' they in the past have asked 'what’s on
your insurance card?' so that instead of saying what’s your legal name it’s just saying
what’s on your insurance card. So that and then..." 4/n
your insurance card?' so that instead of saying what’s your legal name it’s just saying
what’s on your insurance card. So that and then..." 4/n
"The follow up question is "what name can I list
you under?" and "what pronouns can I list for you?" There have been some that have been
really good about that." 5/n
you under?" and "what pronouns can I list for you?" There have been some that have been
really good about that." 5/n
Simon went on to advise that front office staff "not automatically assum[e] voice is intent, so depending on the
office that [I] call, I’ll change my voice if I have to so that I can get through with less problems... upping it, to sound more feminine." 6/n
office that [I] call, I’ll change my voice if I have to so that I can get through with less problems... upping it, to sound more feminine." 6/n
Simon, like all of the participants I interviewed (and trans folks who write about these issues) warned front office staff and form-writers to not use the term "preferred pronouns": "I think preferred implies that this is a choice, that being trans is a choice & it’s not..." 7/n
"Saying preferred is like 'I prefer pepperoni on my pizza, but I’ll eat cheese.' So [making me say] 'I prefer Simon' is extremely diminutive... It puts me into a spot like 'you’re not as worthy as a person'. This is my name. [These are my pronouns]. This is who I am." 8/n
One participant suggested all offices ask "hey, what name can I put in for you?" for EVERYONE because many people's names differ from their legal name. My mother's legal name is Hilda Anne, but she has been Robin since she was a teen. This is a kind of "universal design." 9/n
Other folks asked offices to not have the only options on intake forms for sex/gender be "male", "female", and "other." It can't get more literally Othering than that, eh? Some suggested an "organ inventory" while others found this idea alienating. 10/n
slideplayer.com/slide/12704516/
slideplayer.com/slide/12704516/
Our next positive narrative, from a white trans feminine participant, illustrates a pattern I noticed: Participants were very forgiving of practitioners who tried to do right even if they weren’t there yet, and who put the work in to be supportive and provide good care... 11/n
Asked "Do you think you've found a doctor you can stick with?" she replied, "I like her. She’s new--her words not mine--I’ve seen her twice cuz she wanted to do a follow-up and so I saw her at my initial visit & then I saw her like 30 days ago for a follow up...
12/n
12/n
"...she changed one of my meds and wanted to check it and on one hand there’s been a few times already that I’ve asked a question and she’s like “To be honest, I don’t know. Let me check.”..." 13/n
"On the other hand, the reason that I went out of my way to see her in the first place is I have bottom surgery coming up in January and the surgeon required a health physical. So I had to see a doctor. So obviously I had to tell her why I was seeing her which thus outs me." 14/n
"I was nervous about [outing] but I was actually pleasantly surprised because that’s when she said she was a new doctor & 'I don’t mean that to scare you. I’m hoping it reassures you because after having just gotten out of med school we actually covered some trans health."15/n
"And I was like “oh” [relieved laughter] that’s... you know so for me I would much rather have a doctor that says 'I don’t know, let me get back to you' when I when I ask a question than one that I feel super uncomfortable talking about my gender experience with them."
16/n
16/n
Another participant--49, white, genderqueer & nonbinary--echoed the previous narrative, but with a nurse practitioner rather than a doc who handled her ignorance as with any other patient's condition: by educating themselves and learning more... 17/n
"Yeah so the second I walked in, I actually see his nurse practitioner & I sat in her office & [she says] 'I just came back from a transgender conference to learn more about being culturally competent. I don't know much about genderqueer but I'll look it up.' And she did!" 18/n
"Next time I went in there she was like, like knew more than me. And I was like you are awesome, thank you. And when I got my prescription for the testosterone which did not happen the first time, I got this detailed packet with lots of information..." 19/n
"You know when you're looking for risks & benefits & how it will affect your body the internet is your only source usually & it's not the best source. They had consolidated it & created this pamphlet... It makes me emotional thinking about it. It was like really a kindness." 20/n
This punches me in the ethics every time: "a kindness." Yes, it is a kindness to give people the information they need to made an informed decision in a format that meets what Jay Katz would have called their "informational needs." But it's also a core duty of med ethics. 21/n
Our final narrative brings us back to Jefferson Pierce, the 28 y/o Black non-binary participant who had a terrible time getting care for recurrent throat/tonsil trouble (see yesterday's thread). When asked what their fave doc does that could be replicated, Pierce said... 22/n
"Yeah, he took the time to sit down, to have a conversation with me, to hear what it was that I was looking for, what I needed... I think he mostly just took the time to sit down and hear what it was that I needed. And like, you don’t have to be trans to do that [laughs]." 23/n
"Some of [the questions] I probably could have gotten answered on the internet, but I really just wanted to hear them from a person. He just sat down & asked me are you looking for this, are you looking for [that], what are the effects you’re going for, what is it you need?" 24/n
Pierce's favorite doc was doing less gatekeeping, and more informed consent model, in which what the patient's wants/needs guide the treatment they receive. This doesn't mean doing ANYTHING they want. But it means using their values, their gender, to guide practice. 25/n
Most providers don't know that some trans folks never medically transition even though they socially transition, that others want a little masculinity from testosterone while others want a lot, or a little femininity from estradiol while others want a lot. 26/n
Some trans folks want hormones but no surgery, others want top surgery but not bottom, or any combination. There's no 1 way to be trans,or to interact with healthcare. The patient's other medical conditions and gender should be the guide. Pierce's doc was prepared for that. 27/n
Two participants in the #TransHealthEthicsProject had almost entirely positive experiences. One, a trans man in his 50's, waited all his life to transition. He didn't do it until he had trans-friendly docs all lined up and has stuck with them. His experiences were smooth. 28/n
Another with few negative experiences was a young just-adult trans man who'd grown up with a pediatric trans care unit w/wraparound care & "warm handoffs" to known-trustworthy providers ("Dr. X's office, this is Dr. Y's office. We're sending Jorge over to you next week..."). 29/n
Warm handoffs, a technique often practiced at trans clinics, help to avoid the dehumanizing front office encounters many folks reported. In a hospital setting, staff may actually walk a patient down to radiology/lab and introduce them by their name, modeling pronoun usage. 30/n
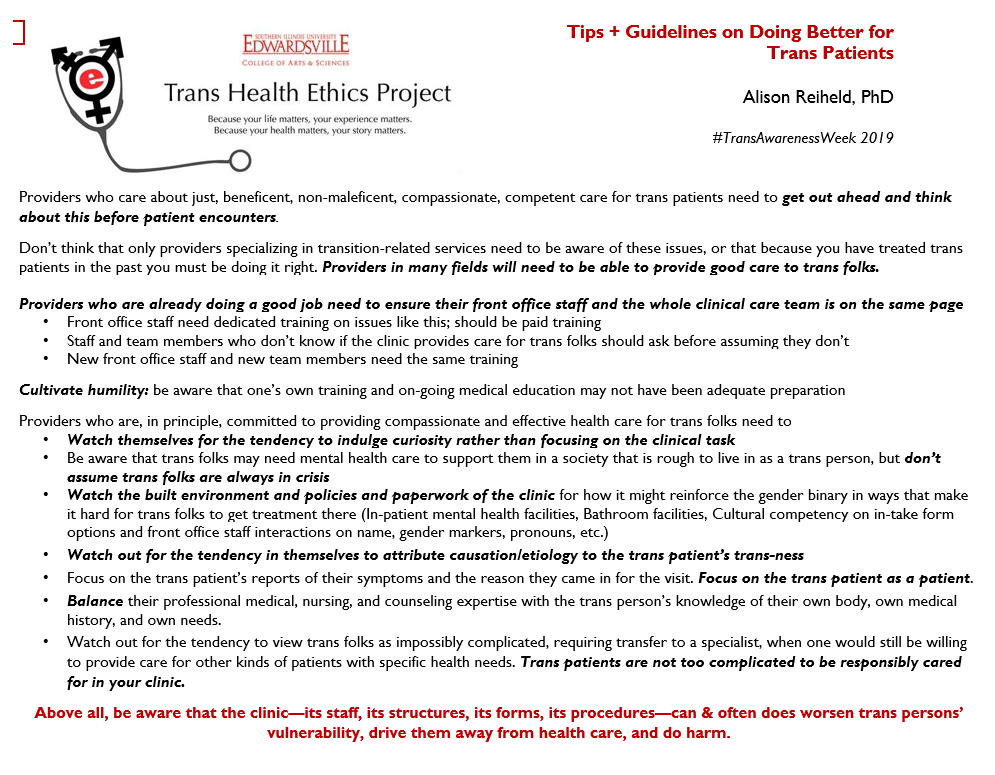
From these negative narratives of health care gone badly & immorally wrong, and positive narratives of health care done well & with ethical sensitivity, we can develop a list of tips/guidelines for ethical care in primary care, specialist, dental, psych, and other settings. 31/n
I'll post these shortly. But why follow them? Because 20% of trans folks report delaying or avoiding necessary preventive AND emergency care because of fear of a repeat of these negative experiences. And providers who don't provide good, timely care aren't being providers. 32/n
Trans folks shouldn't be in the position of having the following health care plan: "My health care plan? To not get sick. That's it. No. It hasn't really worked out." But enough providers are putting trans patients in that position that it is a serious problem. 33/n
The health care trans folks receive when they seek it out determines whether they seek it again. The way a doc or nurse treats them will impact their ability to form relationships with other providers in the future. We can do better at keeping people "in the human club." 34/n
So, here are the tips and guidelines. They boil down to these: treat trans patients as patients; cultivate humility; work on this. Good isn't a thing you are. Good is a thing you do. Let's do better. 35/35
END THREAD
END #TransHealthEthicsProject posts for #TransAwarenessWeek
END THREAD
END #TransHealthEthicsProject posts for #TransAwarenessWeek
@threadreaderapp unroll